
Advances in Animal and Veterinary Sciences


Research Article
Advances in Animal and Veterinary Sciences. 1(2S): 15 – 23Special Issue – 2 (Clinical Veterinary Practice – T rends)
Dexmedetomidine with Butorphanol and Propofol for Total Intravenous Anaesthesia in Uraemic Buffalo Calves
Siddharth Khattri1, Prakash Kinjavdekar2*, Amarpal, Hari Prasad Aithal2, Abhijit Motiram Pawde2, Rohit Kumar3, Jasmeet Singh4
- Private Veterinary Practitioner, Dehradun (Uttrakhand)
- Division of Surgery, Indian Veterinary Research Institute, Izatnagar-243 122, Bareilly (Uttar Pradesh), India
- Division of Surgery, Indian Veterinary Research Institute, Izatnagar-243 122, Bareilly (Uttar Pradesh), India
- Department of Surgery and Radiology, Veterinary College, OUAT, Bhubaneshwar (Odisha)
*Corresponding author: p.kinjavdekar@rediffmail.com
ARTICLE CITATION:
Siddharth Khattri, Prakash Kinjavdekar*, Amarpal, Hari Prasad Aithal, Abhijit Motiram Pawde , Kumar Rohit and Singh Jasmeet (2013). Dexmedetomidine with butorphanol and propofol for total intravenous anaesthesia in uraemic buffalo calves. Adv. Anim. Vet. Sci. 1(2S): 15 – 23.
Received: 2013–11–16, Revised: 2013–12–06, Accepted: 2013–12–09
The electronic version of this article is the complete one and can be found online at
(
http://nexusacademicpublishers.com/table_contents_detail/4/150/html
)
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
ABSTRACT
Sixteen clinical cases of urolithiasis in male buffalo calves of 4–6 months of age and 40–55 kg of weight were used in groups A and B. Group A animals were premedicated with dexmedetomidine (2.5 µg/kg body wt, IV), while in group B dexmedetomidine (2.5 µg/kg body wt, IV) and butorphanol (0.05 mg/kg body wt, IV) were used for premedication. Anaesthesia was induced by 1 % propofol in group A (2.50 ± 0.37 mg/kg) and B (1.99±0.29 mg/kg), and maintained by 1 % propofol with continuous intravenous infusion. A lower dose of propofol for induction and maintenance was required in group B than in group A, whereas recovery time, sternal recumbency time, standing time and duration of anaesthesia were similar in both groups. In both groups, HR and RR decreased significantly (P<0.01)up to 75 min. There was a gradual increase in RR after induction of anaesthesia in both groups, and a significantly higher RR was recorded from 45 to 75 min in group A. Rectal temperature decreased significantly in both groups up to 90 min. Haemoglobin, PCV and TLC decreased in both groups. Significant neutrophilia was recorded in group B and lymphocytopenia in both groups. Urea nitrogen, creatinine and glucose increased in both groups. MAP decreased significantly (P<0.05) after premedication up to the end of observation period in both groups. Decrease in SpO2 after premedication was recorded in both groups. All the animal of both groups recovered without any complications. It was concluded that dexmedetomidine–propofol combination can be used safely for total intravenous anaesthesia in uraemic buffalo calves, however, addition of butorphanol has a dose sparing effect on propofol induction and maintenance anaesthesia in uraemic buffalo calves.
INTRODUCTION
Urolithiasis is a common surgical condition of almost all domestic animals but higher incidence has been recorded in bovine and caprine (Radostits et al., 1994). Several anaesthetic techniques using different drugs have been reported for the management of urolithiasis. Epidural lignocaine hydrochloride (Kinjavdekar et al., 2005), bupivacaine (Singh et al., 2007a), ropivacaine (Singh et al., 2005) and xylazine and ketamine (Singh et al., 2007b) have been used for the anaesthetic management of goats suffering from urolithiasis. General anaesthesia may be preferred over local anaesthesia for any surgical intervention as it provides complete unconsciousness, better insensitivity to pain, good muscle relaxation, and freedom from reflex responses and loss of motor ability (Thurmon et al., 1996). Dexmedetomidine, a newer α2–agonist, reduces the dose requirements of opioids and anaesthetic agents, and attenuates the haemodynamic responses to tracheal intubation and surgical stimuli. Effects of dexmedetomidine have been studied in buffaloes (Singh, 2011), however, there are only a few reports on the use of dexmedetomidine in large ruminants, especially buffaloes. Butorphanol, an opioid agonist–antagonist with sedative and analgesic properties, is known to induce mild sedation accompanied by small decreases in arterial blood pressure, heart rate and arterial oxygen tension in dogs (Trim, 1983). Synergistic interactions have been reported between α2–agonists and opioids or benzodiazepines in earlier studies (Amarpal et al., 1998; Kojma et al., 2002). Synergistic action of butorphanol and dexmedetomidine showed excellent muscle relaxation after anaesthetic induction with propofol in sheep (Monsang, 2011). Propofol, a short–acting hypnotic agent, is usually injected as a single bolus for anaesthetic induction to allow intubation and initiation of inhalant anaesthesia (Short and Bufalari, 1999). Propofol has been investigated as intravenous anaesthetic in sheep (Lin et al., 1997), goats (Amarpal et al., 2002) and buffaloes (Malik et al., 2011). There are no reports available in literature on the use of dexmedetomidine, butorphanol, and propofol for the anaesthetic management of uraemic buffalo calves. Therefore, the present study was designed to compare the suitability of propofol anaesthesia with two different preanaesthetic protocols.
MATERIALS AND METHODS
Sixteen male buffalo calves of 4–6 months of age and 40–55 kg of weight suffering from urolithiasis, brought for treatment to the Referral Veterinary Polyclinic, Indian Veterinary Research Institute, were used. The animals were divided randomly into A and B groups (n=8 each). The animals were restrained in right lateral recumbency and premedicated with intravenous dexmedetomidine (2.5 µg/kg body wt) alone in group A, and dexmedetomidine (2.5 µg/kg body wt) with butorphanol (0.05 mg/kg body wt) in group B. After 10 minutes of premedication, anaesthesia was induced by IV administration of 1 % propofol till effect. Anaesthesia was maintained with continuous intravenous infusion (CII) of propofol. The different treatments were evaluated on the basis of following parameters:
Clinical Observations
Jaw Relaxation
Jaw relaxation was taken as a measure of muscle relaxation and was evaluated at 0, 5, 10, 15, 20, 30, 45, 60, 75, and 90 min intervals by observing the resistance to opening of the jaw on applying pressure on lower and upper jaws, and graded on a 0 to 3 score scale as 0: not allowing to open the jaws, 1: resistant to opening the jaws and closed quickly, 2: less resistance to opening of jaws and closed slowly, and 3: no resistance and jaws remained open. At each interval mean value for jaw relaxation score was calculated and the muscle relaxation was graded as nil on a score of 0, very mild when the score was > 0 but < 1, mild when the score was ≥1 but < 2, moderate when the score was ≥ 2 but < 3 and excellent when the score was 3.
Palpebral Reflex
Palpebral reflex was recorded as a measure of depth of sedation by observing the blink of eye lids on touching the medial canthus with index finger and graded on a 0 to 3 score scale as 0: intact and strong reflex (quick blink), 1: intact but weak reflex (slow response), 2: very weak reflex (very slow and occasional), and 3: abolished reflex. Palpebral reflex was recorded at 0, 5, 10, 15, 20, 30, 45, 60, 75, and 90 min intervals. At each interval mean value for palpebral reflex score was calculated and the sedation was graded as absent on a score of 0, mild when the score was > 0 but < 1, moderate when the score was ≥ 1 but < 2, deep when the score was ≥ 2 but < 3 and very deep when the score was 3.
Pedal Reflex
Pedal reflex was recorded as a measure of depth of analgesia by recording the response to pin prick at coronet region on the digits of hind limbs and graded on a 0 to 3 score scale as 0: intact and strong reflex (strong withdrawal), 1: intact but weak reflex (animal responding slowly), 2: intact but very light reflex (slow and occasional response), and 3: reflex abolished completely. Pedal reflex was recorded at 0, 5, 10, 15, 20, 30, 45, 60, 75 and 90 min intervals. At each interval mean value for pedal reflex score was calculated and the analgesia was graded as no analgesia on a score of 0, very mild analgesia when the score was > 0 but < 1, mild analgesia when the score was ≥ 1 but < 2, moderate analgesia when the score was ≥ 2 but < 3, and complete analgesia when the score was 3.
Salivation
Salivation was recorded at different intervals and graded on a 0 to 3 score scale as 0: No salivation, 1: mild salivation, 2: moderate salivation, and 3: excessive salivation.
Induction
Induction dose of propofol was calculated in mg/kg for each group.
Maintenance
Maintenance dose of propofol was calculated in mg/kg/min for each group.
Recovery Time (RET)
Recovery time (RET) was recorded as the time elapsed from discontinuation of injection of drugs to the reappearance of pedal reflex.
Sternal Recumbency Time (SRT)
Sternal recumbency time (SRT) was recorded as the time elapsed from discontinuation of injection of drugs until the spontaneous regaining of sternal recumbency.
Standing Time (ST)
Standing time (ST) was recorded as the time elapsed from the time of discontinuation of injection of drugs until the spontaneous regaining of standing position and able to walk.
Duration of Anaesthesia
Duration of anaesthesia was recorded as the time elapsed from the time of abolition of pedal reflex to the time of reappearance of pedal reflex.
Urination
Urination and defecation were also recorded.
Physiological Observations
Heart rate (beats/min) by non–invasive blood pressure (NIBP) monitor, respiratory rate (breaths/min) by counting the movement of the thorax, and rectal temperature (oC) by digital thermometer were recorded before administration of drug(s) at 0 minute and at 5, 10, 15, 20, 30, 45, 60, 75 and 90 min after administration of drugs.
Haematological Observations
One ml blood was collected in heparinized (1:1000) disposable syringes, at 0 min (base line), 15, 30, 60 and 90 min after administration of drugs for the estimation of haemoglobin (Hb in g/L) using Sahli’s haemoglobinometer , packed cell volume (PCV in L/L) by microhaematocrit method, total leukocyte count (TLC in X109/L) by using Neubauer counting chamber and differential leukocyte count (DLC in %) by a thin, stained blood smear.
Biochemical Observations
Five ml venous blood was collected in heparinized (1:1000) disposable syringes (1 ml in sodium fluoride for glucose estimation) at 0 min (base line) and at 15, 30, 60 and 90 min after injection of drug(s) for separation of plasma for the estimation of urea nitrogen (mmol/L) by diacetyl monoxide (DAM) method, glucose (mmol/L) by GOD/POD method and creatinine (μmol/L) by alkaline picrate method.
Haemodynamic Observations
Systolic blood pressure (SBP), diastolic blood pressure (DBP) and mean arterial pressure (MAP) were recorded at 0 min (base line) and at 5, 10, 15, 20, 30, 45, 60, 75 and 90 min after administration of the drugs by non invasive blood pressure (NIBP) monitor. Oxygen saturation of haemoglobin (SpO2) by pulse oxymetry was also recorded.
Statistical Analysis
Analysis of Variance (ANOVA) and Duncan’s multiple range test (DMRT) were used to compare the means at different time intervals between the groups. Paired ‘t’ test was used to compare the means at different intervals with respective base values in each group (Snedecor and Cochran, 1994).
RESULTS
Jaw Relaxation
In animals of both groups, the jaws were mildly relaxed after premedication at 5 and 10 min followed by excellent relaxation after induction of anaesthesia up to the end of anaesthetic period (Figure 1). After discontinuation of anaesthesia a normal jaw tone was attained.
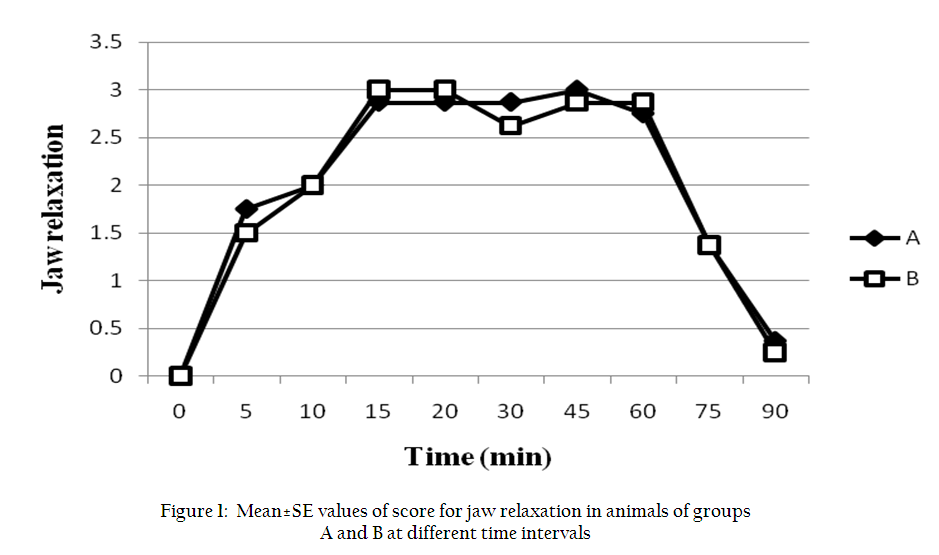
Figure 1: Mean±SE values of score for jaw relaxation in animals of groups A and B at different time intervals
Palpebral Reflex
In animals of group A, the reflex was moderately depressed after premedication at 5 and 10 min, followed by complete abolishion of reflex up to the end of anaesthetic period (Figure.2). In group B, the palpebral reflex was completely abolished from 10 min after premedication up to the end of anaesthesia. Comparison between groups A and B revealed that the palpebral reflex was more depressed in group B.
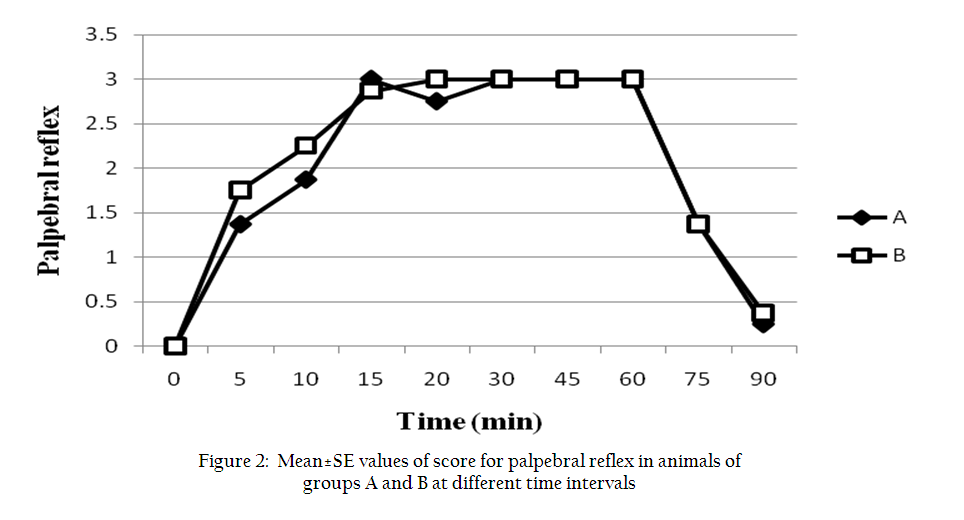
Figure 2: Mean±SE values of score for palpebral reflex in animals of groups A and B at different time intervals
Pedal Reflex
In group A, pedal reflex was mildly depressed after premedication at 5 and 10 min, followed by excellent depression of reflex after induction of anaesthesia up to the end of the anaesthetic period (Figure 3). In animals of group B, pedal reflex was mild to moderately depressed after premedication at 5 and 10 min, followed by excellent depression of reflex up to the end of anaesthetic period.
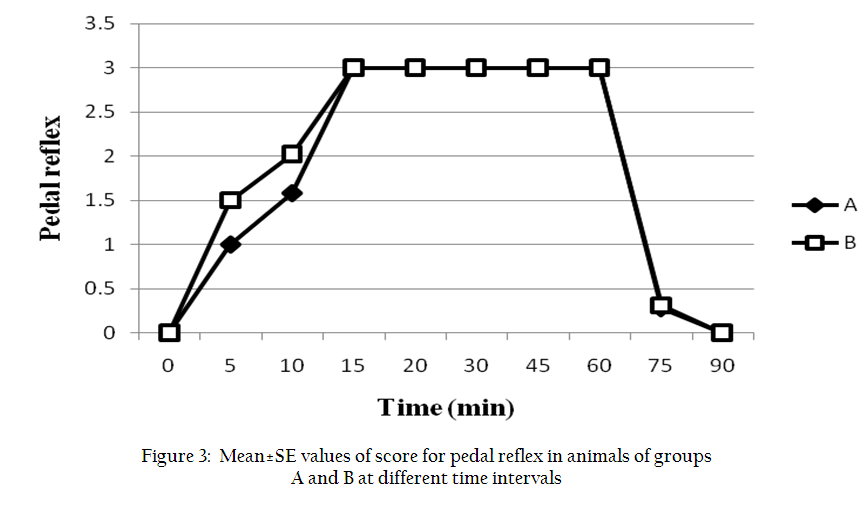
Figure 3: Mean±SE values of score for pedal reflex in animals of groups A and B at different time intervals
Salivation
In animals of group A, a very mild salivation was recorded at premedication followed by a moderate salivation up to the end of anaesthetic period. In group B, a mild salivation was recorded after premedication, which persisted up to the end of anaesthetic period.
Recovery Time
The median ± SD values of recovery time in groups A and B were 5.62±0.62 min and 6.12±.54 min, respectively (Figure 4).
Sternal Recumbency Time
The median ± SD values of sternal recumbency time in groups A and B were 20.87±2.91 min and 21.50±3.02 min, respectively (Figure 4).
Standing Time
The median ± SD values of standing time recorded in groups A and B were 29.75±3.26 min and 29.50±3.13 min, respectively (Figure 4).
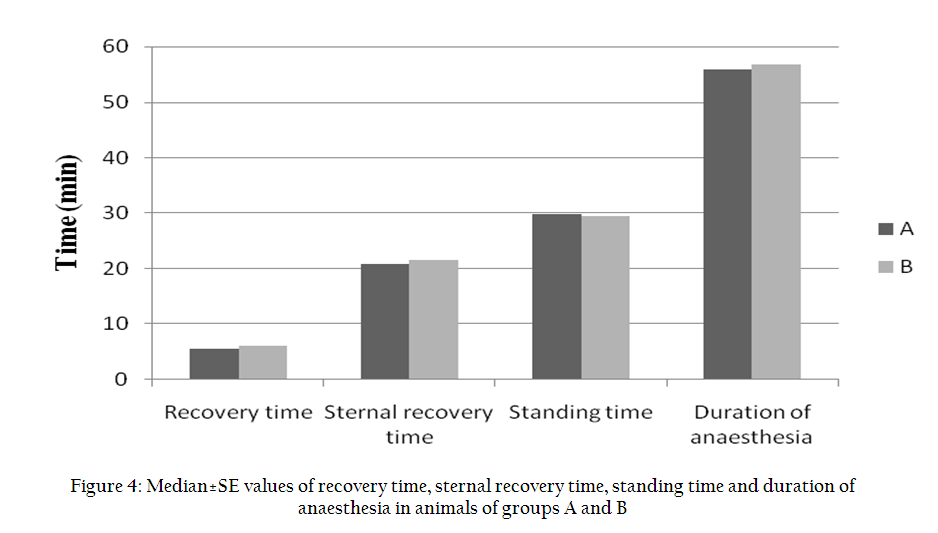
Figure 4: Median±SE values of recovery time, sternal recovery time, standing time and duration of anaesthesia in animals of groups A and B
Duration of Anaesthesia
The median ± SD values of duration of anaesthesia recorded in groups A and B were 55.87±0.95 min and 56.72±1.12 min, respectively (Figure 4).
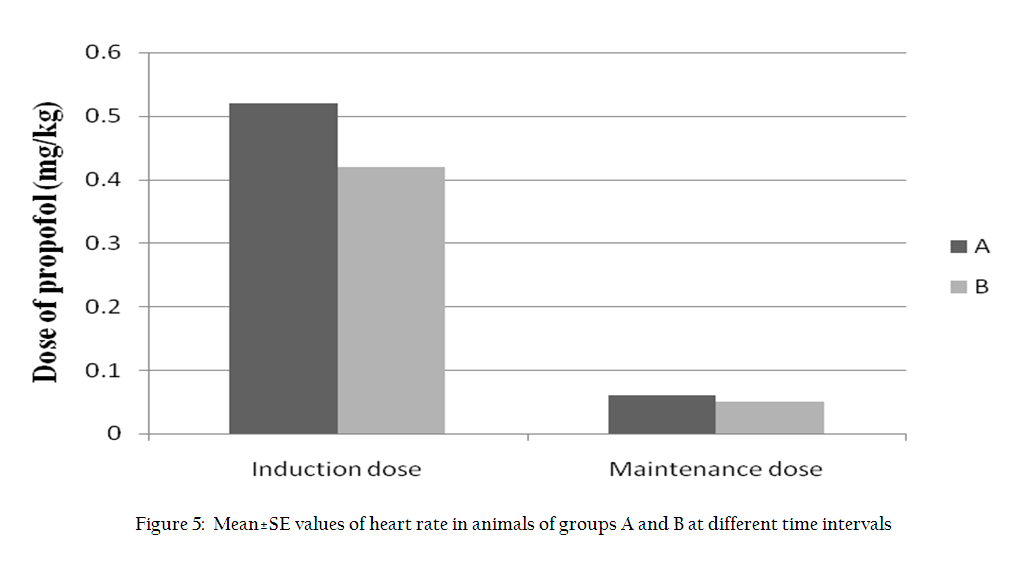
Induction Dose
The mean values of induction dose of propofol required in groups A and B were 0.52+0.08 mg/kg and 0.42+0.06 mg/kg, respectively (Figure 5).
Maintenance Dose
The mean values of maintenance dose of propofol recorded in groups A and B were 0.06+ 0.00 mg/kg/min and 0.05+0.00 mg/kg/min, respectively (Figure 5).
Physiological Observations
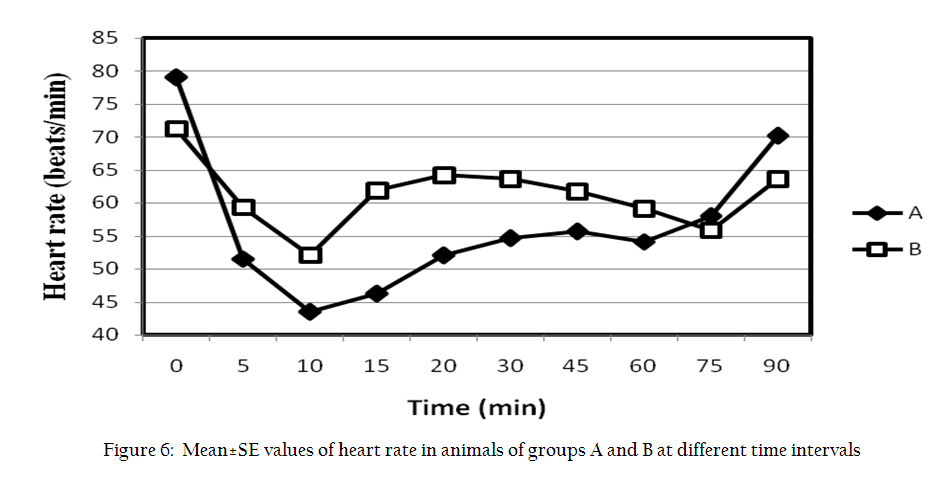
Heart rate (HR): HR decreased (P<0.01) significantly in the animals of group A after premedication. Thereafter, HR improved and remained significantly (P<0.05) below the base line from 20 min to 75 min interval (Figure 6). In the animals of group B, HR decreased significantly (P<0.01) following premedication. A slight increase in HR was recorded after induction, however, the values remained significantly (P<0.05) decreased from the base line till the end of observation period.
Respiratory Rate (RR)
RR decreased (P<0.05) significantly after premedication in both groups but after induction it increased significantly (P<0.01) in group A from 45 to 75 min (Figure 7). In group B, there was a gradual increase in RR after induction of anaesthesia and it remained above the base line up to the end of observation period.
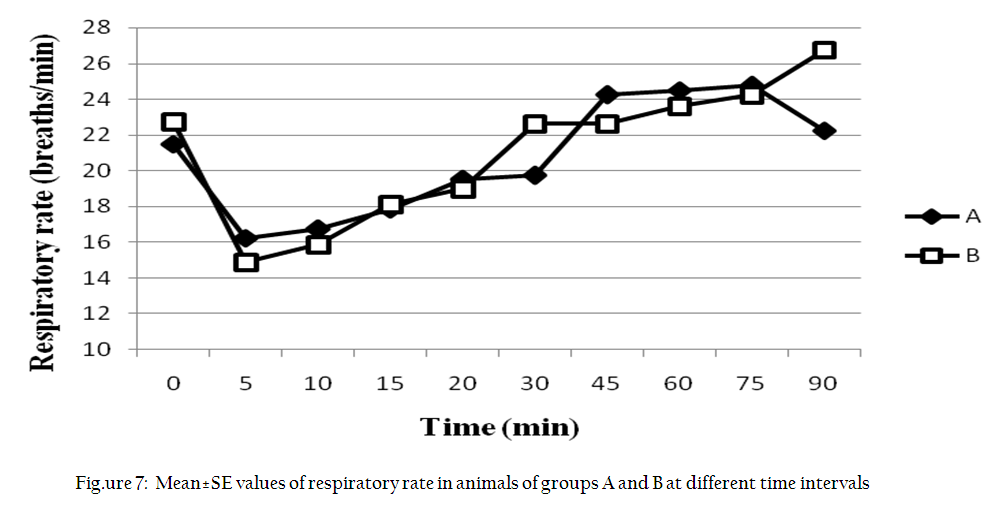
Figure 7: Mean±SE values of respiratory rate in animals of groups A and B at different time intervals
Rectal Temperature (RT)
In group A, RT decreased significantly (P<0.01) in both groups during almost the entire observation period (Figure 8).
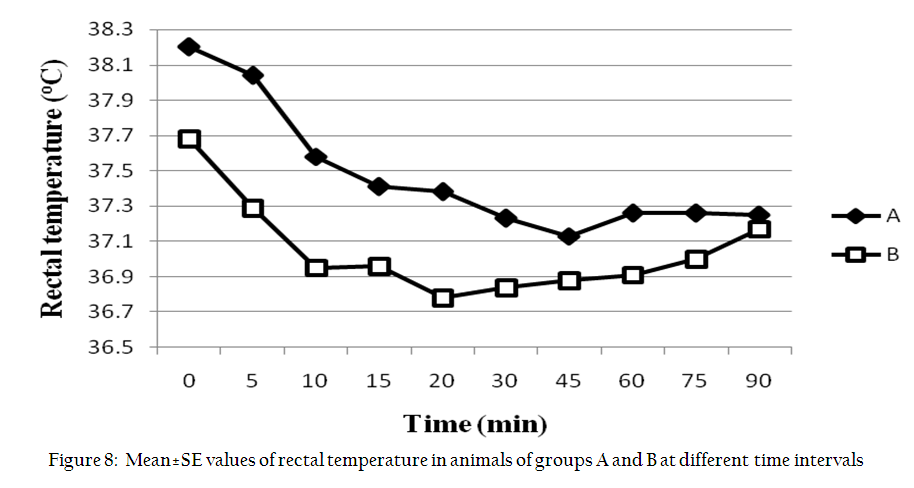
Figure 8: Mean±SE values of rectal temperature in animals of groups A and B at different time intervals
Haematological Observations
Haemoglobin (Hb), Packed Cell Volume (PCV) and Total leukocyte count (TLC)
In both groups, there was a significant (P<0.01) decrease in Hb, PCV and TLC from 15 to 90 min (Table).
Neutrophils and Lymphocytes
In both groups there was a significant (P<0.01) increase in neutrophils and corresponding decrease in lymphocytes from 15 to 90 min of observation period (Table).
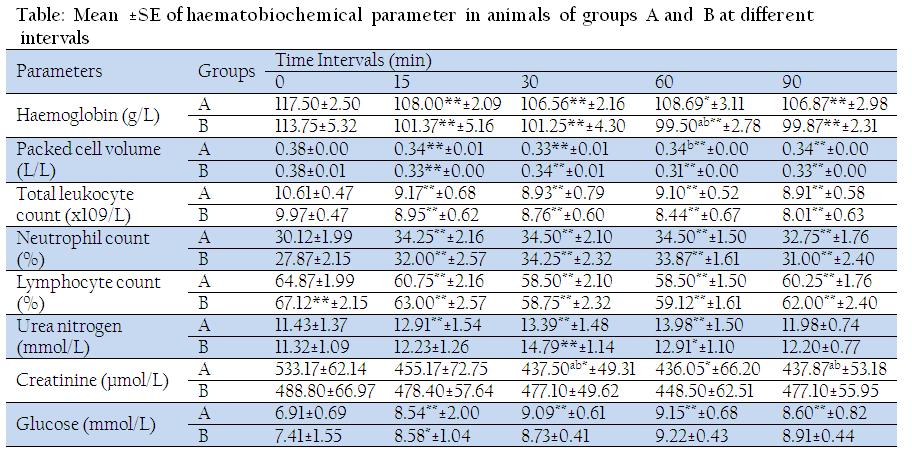
Table: Table: Mean ±SE of haematobiochemical parameter in animals of groups A and B at different intervals
Biochemical Observations
Urea nitrogen: In group A the urea nitrogen increased significantly (P<0.01) from 15 to 60 min of observation period (Table). In group B, urea nitrogen increased significantly (P<0.01) at 30 min and 60 min (P<0.05).
Glucose
In group A, glucose increased significantly (P<0.01) from 15 min to 90 min of observation period (Table). In group B, glucose increased significantly (P<0.05) at 15 min. From 30 min of observation period, the plasma glucose started decreasing to return to its base level by 90 min.
Creatinine
In group A, creatinine decreased significantly (P<0.05) from 15 min up to the end of the observation period (Table). In group B, creatinine decreased (P<0.05) significantly at 15 min.
Haemodynamic Observations
Systolic blood pressure (SBP) and Diastolic blood pressure (DBP): SBP and DBP decreased significantly (P<0.01) after premedication up to 90 min of observation in both groups.
Mean Arterial Blood Pressure (MAP)
In group A, a more significant (P<0.01) decrease in MAP from premedication up to 75 min of observation was recorded except at 90 min where the decrease was less significant (P<0.05) (Figure 9). In group B, a significant (P<0.01) decrease in MAP was recorded throughout the period of observation.
MAP was significantly (P<0.05) lower in group B as compared to that in group A at 75 min.

Figure 9: Mean±SE values of mean arterial pressure in animals of groups A and B at different time intervals
Haemoglobin Oxygen Saturation (SpO2)
In group A, a significant (P<0.05) decrease in SpO2 at 15 min and 20 min and a highly significant (P<0.01) decrease from 30 to 60 min was recorded (Figure 10). In group B, a significant (P<0.01) decrease in SpO2 was recorded from premedication up to 15 min of observation period.
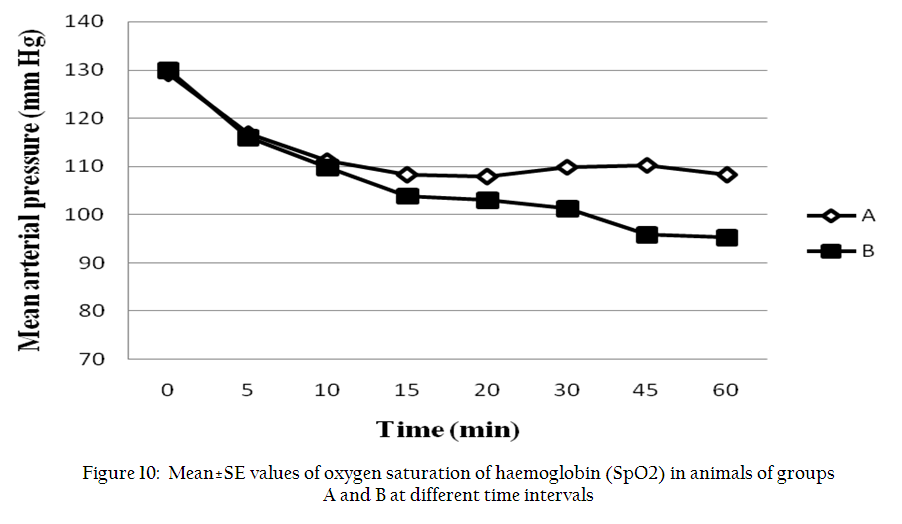
Figure 10: Mean±SE values of oxygen saturation of haemoglobin (SpO2) in animals of groups A and B at different time intervals
DISCUSSION
The jaw relaxation was excellent at most of the intervals in both groups. Alpha 2–adrenergic agonists have been reported to produce profound muscle relaxation when used alone or in combination with opioid agonist–antagonists (Ko et al., 1996; Pratap et al., 2000; Ahmad et al, 2011; Singh, 2011). The muscle relaxation effect that accompanies sedation is due to inhibition of alpha 2–adrenoceptors at the interneuron level of the spinal cord (Cullen, 1996). Excellent muscle relaxation recorded after induction with propofol in the present study might be due to combined effects of alpha 2–agonist, opioid and propofol.
Dexmedetomidine induces a dose dependent sedation but increasing the dose beyond a certain level does not cause a further increase in sedation (Kuusela et al., 2000). Synergistic sedative and analgesic activity between alpha 2–agonist and opioid agonist–antagonist has been reported in ruminants (Malik et al., 2011; Singh, 2011). In the present study, mild to moderate analgesia recorded in both groups during preanaesthetic period might be due to administration of dexmedetomidine and butorphanol. However, excellent analgesia observed after administration of propofol might be due to the action of anaesthetic propofol.
The reduction in the induction dose of propofol in group B than in group A might be due to synergistic action of dexmedetomidine and butorphanol. A marked synergism between alpha 2–agonists and propofol has been reported previously (Hammond and England, 1994). Synergism between alpha 2–agonists, butorphanol and propofol might have played an important role in reducing the induction and maintenance dose of propofol in group B in the present study.
Rapid recovery after propofol and halothane anaesthesia has been reported in goats (Carroll et al., 1998). Similar findings were also observed in the present study. There is lack of any cumulative effect of propofol after its administration either by repeat bolus injection or by continuous infusion (Adetunji et al., 2002).
Bradycardia has been reported following dexmedetomidine administration in goats (Kastner et al., 2005) and sheep (Kastner et al., 2006; Monsang, 2011). Butorphanol has been reported to produce mild lowering of HR and minimum cardiovascular effects (Greene et al., 1990). It has also been reported that butorphanol facilitates the increase in parasympathetic tone and thereby contributes to bradycardia (Ko et al., 2000). Bradycardia recorded in the present study could be attributed to the action of dexmedetomidine and butorphanol.
The initial reduction in RR recorded in the present study might be due to dexmedetomidine and butorphanol. More reduction in RR recorded in group B was in accordance with the earlier studies where a greater respiratory depression was recorded when medetomidine was combined with butorphanol in buffaloes (Malik et al., 2011). Similarly, decreased RR was reported following administration of dexmedetomidine along with butorphanol in dogs (Gupta, 2010; Surbhi et al., 2010), sheep (Monsang, 2011) and buffaloes (Ahmad, 2009). Propofol caused a further decrease in mean RR in groups A and B, plausibly by depressing central inspiratory drive and ventilatory response to arterial carbon–dioxide response (Goodman et al., 1987).
A decrease in RT recorded in both groups might be attributed to a decrease in the skeletal muscle tone, reduced metabolic rate and muscle relaxation along with depression of thermoregulatory centers. Alpha–2 adrenergic agonists have been reported to induce prolonged depression of thermoregulation (Ponder and Clarke, 1980). These agents have also been found to depress hypothalamic noradrenergic alpha 2 receptors to cause hypothermia (MacDonald et al., 1988). Decrease in RT has been reported after dexmedetomidine in dogs (Ahmad et al., 2011; Santhosh, 2011) and sheep (Monsang, 2011), and dexmedetomidine and butorphanol in dogs (Gupta, 2010) and sheep (Monsang, 2011). Hypothermia has also been reported during propofol anaesthesia in goats (Carroll et al., 1998; Amarpal et al., 2002) and buffaloes (Malik et al., 2011).
Haemoglobin, PCV and TLC decreased significantly in both groups during post–anaesthetic period. Pooling of circulatory blood cells in the spleen or other reservoirs secondary to decreased sympathetic activity may explain the decrease in Hb, PCV and TLC (Wagner et al., 1991). The decrease in PCV and Hb during the period of anaesthesia or sedation may also be due to shifting of fluid from extravascular compartment to intravascular compartment in order to maintain normal cardiac output in the animals (Wagner et al., 1991). The decreased Hb and PCV have also been reported after administration of dexmedetomidine in dogs (Gupta, 2010) and sheep (Monsang, 2011), butorphanol alone (Ahmad, 2009) and along with midazolam in buffaloes (Malik et al., 2011). Neutrophilia and lymphocytopenia recorded in the present study might be due to the stress caused by the preanaesthetic and anaesthetic drugs and subsequent stimulation of adrenal glands. Similar findings have been reported after administration of dexmedetomidine in dogs (Ahmad et al., 2011) and sheep (Monsang, 2011), or combinations of dexmedetomidine–midazolam–fentanyl in dogs (Ahmad et al., 2011), midazolam–butorphanol in sheep (Monsang, 2011), butorphanol–medetomidine or butorphanol–halothane in buffaloes (Malik et al., 2011).
The increase in urea nitrogen might be attributed to the temporary inhibitory effects of anaesthetic drugs on the renal blood flow, which in turn might have caused a rise in urea nitrogen level as suggested by Kinjavdekar et al. (2000). The increased hepatic urea production from amino acid degradation could also account for the observed increase in blood urea values during the maximum depth of anaesthesia (Eichner et al., 1979). Increased BUN has been recorded during propofol anaesthesia in dogs premedicated with xylazine (Surbhi et al., 2010).
The increase in plasma glucose observed in the present study might be attributed to an alpha 2–adrenergic inhibition of insulin release from beta cells of pancreas and increased glucose production in the liver (Gasthuys et al., 1987). Increased glucose has also been reported following administration of medetomidine/dexmedetomidine–butorphanol followed by propofol anaesthesia in canine orthopaedic patients (Gupta, 2010), buffaloes (Malik et al., 2011) and sheep (Monsang, 2011), or propofol in dogs (Surbhi et al., 2010; Ahmad et al., 2011).
Dexmedetomidine might have been responsible for adequate renal blood flow and enough glomerular filtration rate to maintain creatinine near the base value in both groups. However, creatinine was reported to increase following administration of butorphanol–xylazine (Surbhi et al., 2010) or medetomidine in propofol anaesthetized canine orthopaedic patients (Gupta, 2010; Surbhi et al., 2010) and healthy buffaloes (Ahmad, 2009; Malik et al., 2011).
Decreased blood pressure after premedication might be attributed to the effects of dexmedetomidine as IV administration of alpha–2 agonists have been reported to cause a prolonged hypotension (Ruffolo et al., 1993). Hypotension is also attributed to bradycardia and vasodilation, stimulation of central alpha–2 adrenoceptors, peripheral sympatholytic action and enhanced parasympathetic outflow (Tibirica et al., 1991). Decreased BP has been reported following administration of medetomidine–butorphanol during halothane anaesthesia in buffaloes (Ahmad, 2009; Malik et al., 2011). A decrease in blood pressure after propofol administration has been associated with arterial and venous vasodilatation and decreased contractility of the heart (Ilkiw et al., 1992).
Decrease in SpO2 was possibly due to a certain degree of respiratory depression in both groups. Detomidine, medetomidine and romifidine produce severe hypoxaemia when administered IV at equipotent sedative doses in conscious sheep (Celly et al., 1997a, 1997b). Similarly, decreased SpO2 has been reported following administration of butorphanol–medetomidine or dexmedetomidine in propofol anaesthetized dogs (Gupta, 2010; Surbhi et al., 2010) and sheep (Monsang, 2011). Propofol infusion has been reported to cause significant respiratory depression with decrease in all measures of ventilation in animals (Kuusela et al., 2003).
Based on the present study, it is concluded that dexmedetomidine (2.5µg/kg) induces good sedation, analgesia and muscle relaxation in uraemic buffalo calves but causes transient cardiopulmonary depression. Butorphanol can augment sedation and analgesia produced by dexmedetomidine, and can spare the dose of propofol needed for induction and maintenance of anaesthesia.
REFERENCES
Adetunji A, Ajadi RA, Adewoye CO and Oyemakinde BO (2002). Total intravenous anaesthesia with propofol: Repeat bolus versus continuous propofol infusion techniques in xylazine premedicated dogs. J. Israel Vet. Med. Assoc. 57: 139–144.
Ahmad R (2009). Evaluation of halothane anaesthesia following induction with propofol or thiopental in acepromazine/medetomidine–butorphanol premedicated buffaloes. M.V.Sc. Thesis submitted to Deemed University, Indian Veterinary Research Institute, Izatnagar (U.P.), India.
Ahmad RA, Amarpal, Kinjavdekar P, Aithal HP, Pawde AM and Kumar D (2011). Effects of midazolam or midazolam–fentanyl on sedation and analgesia produced by intramuscular dexmedetomidine in dogs. Asian J. Anim. Sci. 5: 302–316.
http://dx.doi.org/10.3923/ajas.2011.302.316
Amarpal, Aithal HP, Pratap K and Singh GR (1998). Neuroleptanalgesia with medetomidine and pentazocine in goats. Indian Vet. J. 75: 150–154.
Amarpal, Kinjavdekar P, Aithal HP, Pawde AM and Pratap K (2002). Analgesic, sedative and haemodynamic effects of spinally administered romifidine in female goats. J. Vet. Med. (A) 49: 3–8.
http://dx.doi.org/10.1046/j.1439-0442.2002.00385.x
Blood, DC and Radostits OM 1994. Veterinary Medicine. 8th ed. Bailliere Tindall, London. PMCid:PMC44623
Carroll GL, Hooper RN, Slater MR, Hartsfield SM and Matthews NS (1998). Detomidine–butorphanol–propofol for carotid artery translocation and castration or ovariectomy in goats. Vet. Surg. 27: 75–82.
http://dx.doi.org/10.1111/j.1532-950X.1998.tb00101.x
PMid:9449181
Celly CS, McDonell WN, Black WD and Young CS (1997a). Cardiopulmonary effects of clonidine, diazepam and the peripheral alpha 2–adrenoceptor agonist ST–91 in conscious sheep. J. Vet. Pharmacol. Therap. 20: 472–478.
http://dx.doi.org/10.1046/j.1365-2885.1997.00098.x
PMid:9430771
Celly CS, McDonell WN, Young SS and Black WD (1997b). The comparative hypoxaemic effect of four alpha 2–adrenoceptor agonists (xylazine, romifidine, detomidine and medetomidine) in sheep. J. Vet. Pharmacol. Therap. 20: 464–471.
http://dx.doi.org/10.1046/j.1365-2885.1997.00097.x
PMid:9430770
Cullen LK (1996). Medetomidine sedation in dogs and cats: a review of its pharmacology, antagonism and dose. Br. Vet. J. 152: 519–535.
http://dx.doi.org/10.1016/S0007-1935(96)80005-4
Eichner RD, Proir RL and Kvascnicka WG (1979). Xylazine induced hyperglycemia in beef cattle. Am. J. Vet. Res. 40: 127–129.
PMid:453674
Gasthuys F, Terpstra P, Hende CV and DeMoor A (1987). Hyperglycemia and diuresis during sedation with detomidine in the horse. J. Am. Vet. Med. Assoc. 34: 641.
http://dx.doi.org/10.1111/j.1439-0442.1987.tb00326.x
Goodman NW, Black AM S and Carter JA (1987). Some ventilatory effects of propofol as sole anaesthetic agent. Br. J. Anaesth. 59: 1497–1503.
http://dx.doi.org/10.1093/bja/59.12.1497
PMid:3122806
Greene SA, Hartsfield SM and Tyner CL (1990). Cardiovascular effects of butorphanol in halothane anaesthetized dogs. Am. J. Vet. Res. 8: 1276–1279.
Gupta AN (2010). Evaluation of medetomidine and dexmedetomidine with propofol for TIVA and tramadol and fentanyl for analgesic management of canine orthopaedic patients. M.V.Sc. Thesis submitted to Deemed University, Indian Veterinary Research Institute, Izatnagar (U.P.), India.
Hammond RA and England GCW (1994). The effect of medetomidine premedication upon propofol induction and infusion anaesthesia in the dog. J. Assoc. Vet. Anaesthetists. 21: 24–28.
http://dx.doi.org/10.1111/j.1467-2995.1994.tb00478.x
Ilkiw JE, Pascoe PJ, Haskins SC and Patz JD (1992). Cardiovascular and respiratory effects of propofol administration in hypovolemic dogs. Am. J. Vet. Res. 53: 2323–2327.
PMid:1476316
Kastner SB, Kull S, Kutter APN, Boller J, Bettschart–Wolfensberger R and Huhtinen MK (2005). Cardiopulmonary effects of dexmedetomidine in sevoflurane anesthetized sheep with or without nitric oxide inhalation. Am. J. Vet. Res. 66:1496–1502.
http://dx.doi.org/10.2460/ajvr.2005.66.1496
PMid:16261821
Kastner SB, Kutter AP, Von–Rechenberg B and Bettschart–Wolfensberger R (2006). Comparison of two pre–anaesthetic medetomidine doses in isoflurane anaesthetized sheep. Vet. Anaesth. Analg. 33: 8–16.
http://dx.doi.org/10.1111/j.1467-2995.2005.00230.x
PMid:16412127
Kinjavdekar P, Amarpal, Aithal HP, Pawde AM, Pratap K, Singh T and Singh K (2005). Management of urolithiasis in goats (Capra hircus): A retrospective study of 25 cases. Indian J. Anim. Res. 39: 8–13.
Kinjavdekar P, Singh GR, Amarpal, Aithal HP and Pawde AM (2000). Physiologic and biochemical effects of subarachnoidally administered xylazine and medetomidine in goats. Small Rum. Res. 38: 217–228.
http://dx.doi.org/10.1016/S0921-4488(00)00161-9
Ko JCH, Bailey JE, Pablo LS and Heaton–Jones TG (1996). Comparison of sedative and cardiorespiratory effects of medetomidine and medetomidine–butorphanol combination in dogs. Am. J. Vet. Res. 57: 535–540.
PMid:8712521
Ko JC, Fox SM and Mandsager RE (2000). Sedative and cardiorespiratory effects of medetomidine, medetomidine–butorphanol, and medetomidine–ketamine in dogs. J. Am. Vet. Med. Assoc. 216: 1578–1583.
http://dx.doi.org/10.2460/javma.2000.216.1578
PMid:10825944
Kojima K, Nishimura R, Mutoh T, Hong SH, Mochizuki M and Sasaki N (2002). Effects of medetomidine–midazolam, acepromazine–butorphanol, and midazolam–butorphanol on induction dose of thiopental and propofol and on cardiopulmonary changes in dogs. Am. J. Vet. Res. 63: 1671–1679.
http://dx.doi.org/10.2460/ajvr.2002.63.1671
PMid:12492281
Kuusela E, Raekallio M, Anttila M, Flack I, Mosla S and Vainio O (2000). Clinical effects and pharmacokinetics of medetomidine and its enantiomers in dogs. J. Vet. Pharmacol. Therap. 23: 15–20.
http://dx.doi.org/10.1046/j.1365-2885.2000.00245.x
PMid:10747239
Kuusela E, Vainio O, Short CE, Leppaluoto J, Huttunen P, Strom S, Huju V, Valtonen A and Raekallio M (2003). A comparison of propofol infusion and propofol isoflurane anaesthesia in dexmedetomidine premedicated dogs. J. Vet. Pharmacol. Therap. 26: 199–204.
http://dx.doi.org/10.1046/j.1365-2885.2003.00465.x
PMid:12755904
Lin HC, Purohit RC and Powe TA (1997). Anaesthesia in sheep with propofol or with xylazine –ketamine followed by halothane. Vet. Surg. 26: 247–252.
http://dx.doi.org/10.1111/j.1532-950X.1997.tb01494.x
PMid:9150564
MacDonald E, Scheinin H and Schienin M (1988). Behavioural and neurological effects of medetomidine, a novel veterinary sedative. Eur. J. Pharmacol. 158: 119–127.
http://dx.doi.org/10.1016/0014-2999(88)90260-9
Malik V, Kinjavdekar P, Amarpal, Aithal HP, Pawde AM and Surbhi (2011). Sedative, analgesic, cardiopulmonary and haemodynamic effects of medetomidine–butorphanol and midazolam–butorphanol on thiopental–propofol anaesthesia in water buffaloes (Bubalus bubalis). J. Appl. Anim. Res. 39: 284–287.
http://dx.doi.org/10.1080/09712119.2011.607715
Monsang SW (2011). Comparison of medetomidine and dexmedetomidine with and without butorphanol and midazolam as preanaesthetics to propofol anaesthesia in sheep. PhD Thesis, Indian Veterinary Research Institute, Izatnagar (U.P.), India.
Pawde AM, Amarpal, Singh GR and Kumar N (1996). Clinicophysiological effects of medetomidine in female goats. Small Rum. Res. 20: 95–98.
http://dx.doi.org/10.1016/0921-4488(95)00784-9
Ponder SW and Clarke WG (1980). Prolonged depression of thermoregulation after xylazine administration to cats. J. Vet. Pharmacol. Therap. 3: 203–207.
http://dx.doi.org/10.1111/j.1365-2885.1980.tb00483.x
Pratap K, Amarpal, Kinjavdekar P and Singh GR (2000). Effects of medetomidine alone or in combination with ketamine on analgesia, physiological parameters and blood values of buffalo calves (Bubalus bubalis). Phillip. J. Vet. Med. 37: 38–40.
Ruffolo RRJr, Nichols AJ and Stadel JM (1993). Pharmacological and therapeutic applications of alpha–2 adrenoceptor subtypes. Annual Rev. Pharmacol. Toxicol. 32: 24–279.
Santosh KM (2011). Evaluation of dexmedetomidine as preanaesthetic to ketamine anaesthesia in midazolam or midazolam–fentanyl premedicated dogs. MVSc thesis submitted to Deemed University IVRI, Izatnagar (U.P.), India.
Short CE and Bufalaria A (1999). Propofol anesthesia. Vet. Clin. North Am. Small Anim. Pract., 29: 747–778.
PMid:10332821
Sinclair MD (2003). A review of the physiological effects of alpha 2–agonists related to the clinical use of medetomidine in small animal practice. Can. Vet. J. 44: 885–897.
PMid:14664351 PMCid:PMC385445
Singh GD (2011). Comparative evaluation of halothane and isoflurane inhalation anaesthesia in buffaloes. Ph.D. Thesis submitted to Deemed University, Indian Veterinary Research Institute, Izatnagar (U.P.), India.
Singh K, Kinjavdekar P, Amarpal, Aithal HP, Gopinathan A, Singh GR, Singh T, Pawde AM and Pratap K (2005). Clinico–physiological and haematobiochemical effects of epidural ropivacaine in uraemic and healthy caprines. Indian J. Vet. Surg. 26: 11–15.
Singh K, Kinjavdekar P, Amarpal, Aithal HP, Gopinathan A, Singh GR, Pawde AM and Pratap K (2007a). Comparison of the analgesic, clinicophysiological and haematobiochemical effects of epidural bupivacaine in healthy and uraemic goats. Small Rum. Res.71, 13–20.
http://dx.doi.org/10.1016/j.smallrumres.2006.02.009
Singh K, Kinjavdekar P, Amarpal, Aithal HP, Gopinathan A, Singh GR, Pawde AM and Pratap K (2007b). Effects of epidural ketamine and xylazine combination on the clinicophysiological and haematobiochemical parameters of uraemic and healthy goats. Vet. Res. Com. 31: 133–142.
http://dx.doi.org/10.1007/s11259-006-3367-4
PMid:17216318
Snedecor GW and Cochran WG (1980). Statistical methods. 9th edn., Iowa State University, Press.
Surbhi, Kinjavdekar P, Amarpal, Aithal HP, Pawde AM, Pathak, M and Borena BM (2010). Physiological and biochemical effects of medetomidine–butorphanol–propofol anaesthesia in dogs undergoing orthopaedic surgery. Indian J. Vet. Surg. 31: 101–104.
Thurmon JC, Ko JCH, Benson GJ, Tranquilli WJ and Olson WA (1996). Hemodynamics and analgesic effects of propofol infusion in medetomidine–premedicated dogs. Am. J. Vet. Res. 55: 363–367.
Tibirica E, Feldman J, Mermet C, Gonon F and Bousquet P (1991). An imidazoline– specific mechanism for the hypotensive effects of clonidine: a study with yohimbine and idazoxan. J. Pharmacol. Exp. Therap. 256: 606–613.
PMid:1671597
Trim CM (1983). Cardiopulmonary effects of butorphanol tartrate in dogs. Am. J. Vet. Res. 44: 329–331.
PMid:6830022
Wagner AE, Muir WW III and Hinchcliff KW (1991). Cardiovascular effects of xylazine and detomidine in horses. Am. J. Vet. Res. 52: 651–657.
PMid:1854087

