

Left Circumflex Coronary Artery to Bronchial Arterial Fistula Associated with Tetralogy of Fallot: A Case Report and Review of Literature




Left Circumflex Coronary Artery to Bronchial Arterial Fistula Associated with Tetralogy of Fallot: A Case Report and Review of Literature
Zunping Ke1, Chao Li2, Qiang Liu3, Gang Bai4, Junfeng Wang5, Ming Zhou5 and Xiao Dong5,*
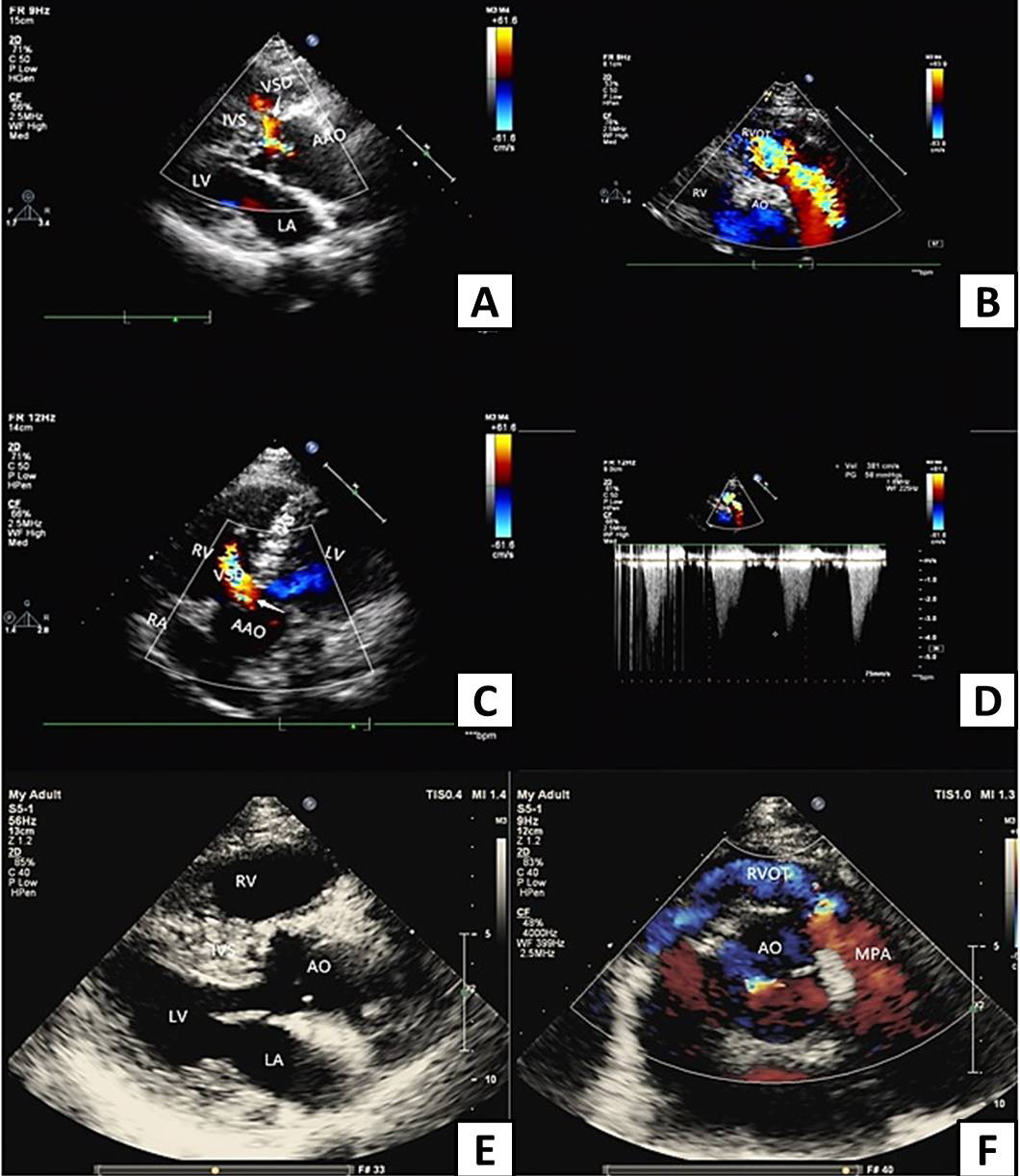
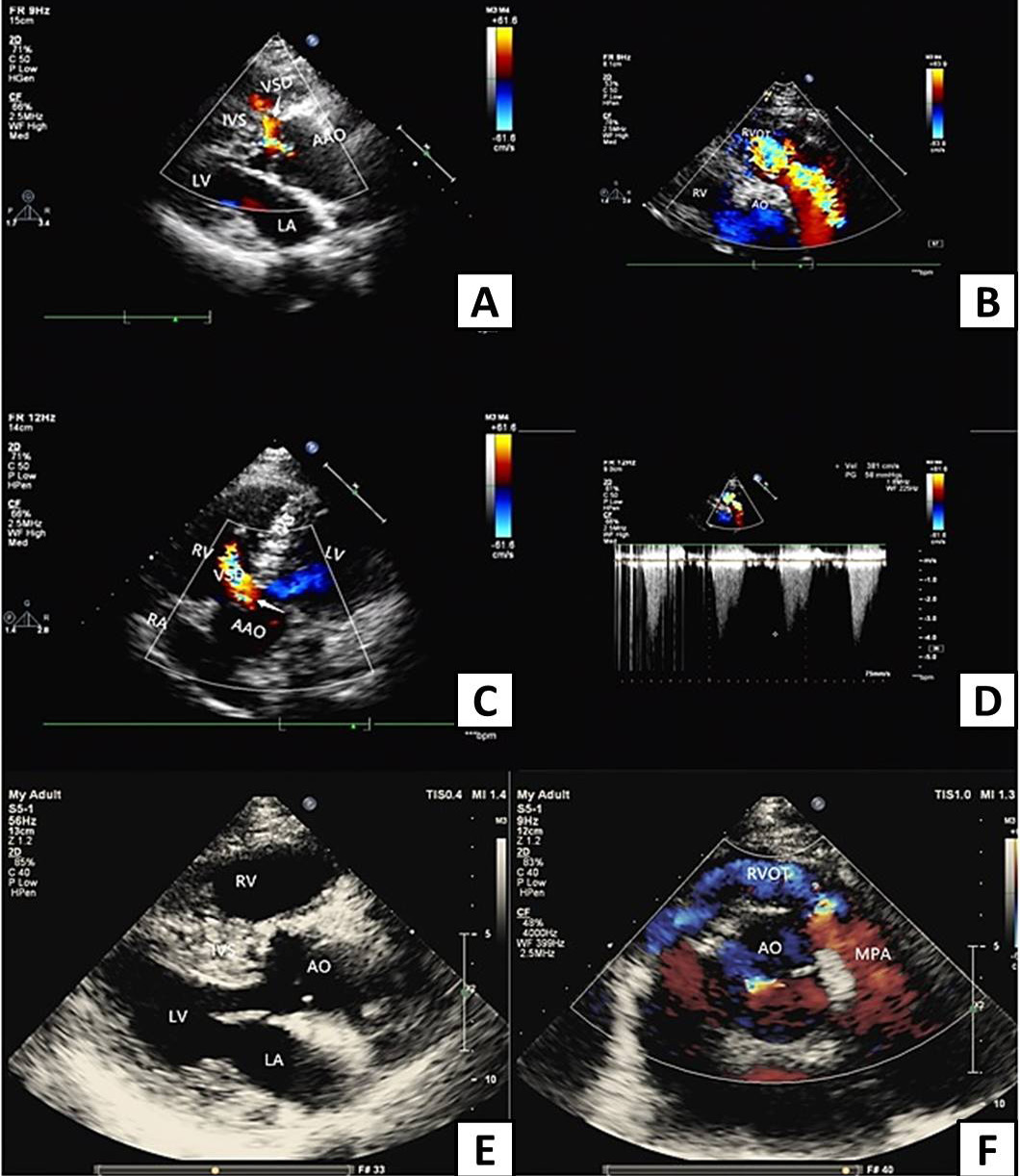
Transthoracic echocardiography before and after corrective surgery (AAO, ascending aorta. AO, aorta; RVOT, right ventricular outflow tract; VSD, ventricular septal defect; IVS, interventricular septum; RA, right atrium; LA, left atrium; RV, right ventricle; LV, left ventricle). A, Parasternal long axis view of left ventricle shows interruption of ventricular septum continuity before surgery, arrow points to left to right shunt of ventricular defect. B, Nonstandard axis view shows obvious acceleration of right ventricular outflow tract blood flow with multicolored mosaic blood flow signals before surgery. C, Apical 5-chamber view shows interruption of ventricular septum continuity before surgery, arrow points to left to right shunt of ventricular defect. D, Color doppler flow diagram of right ventricular outflow tract before surgery, the blood flow of right ventricular outflow tract was obviously accelerated, the peak systolic velocity was about 3.8 m/s, and the pressure difference was 54 mmHg. E, Long axis view of the left ventricle shows RVH, closure of the VSD and RVOT augmentation after corrective surgery. F, The short axis view of the aorta shows the blood flow of right ventricular outflow tract was nearly normal after corrective surgery, no blood flow acceleration was found.
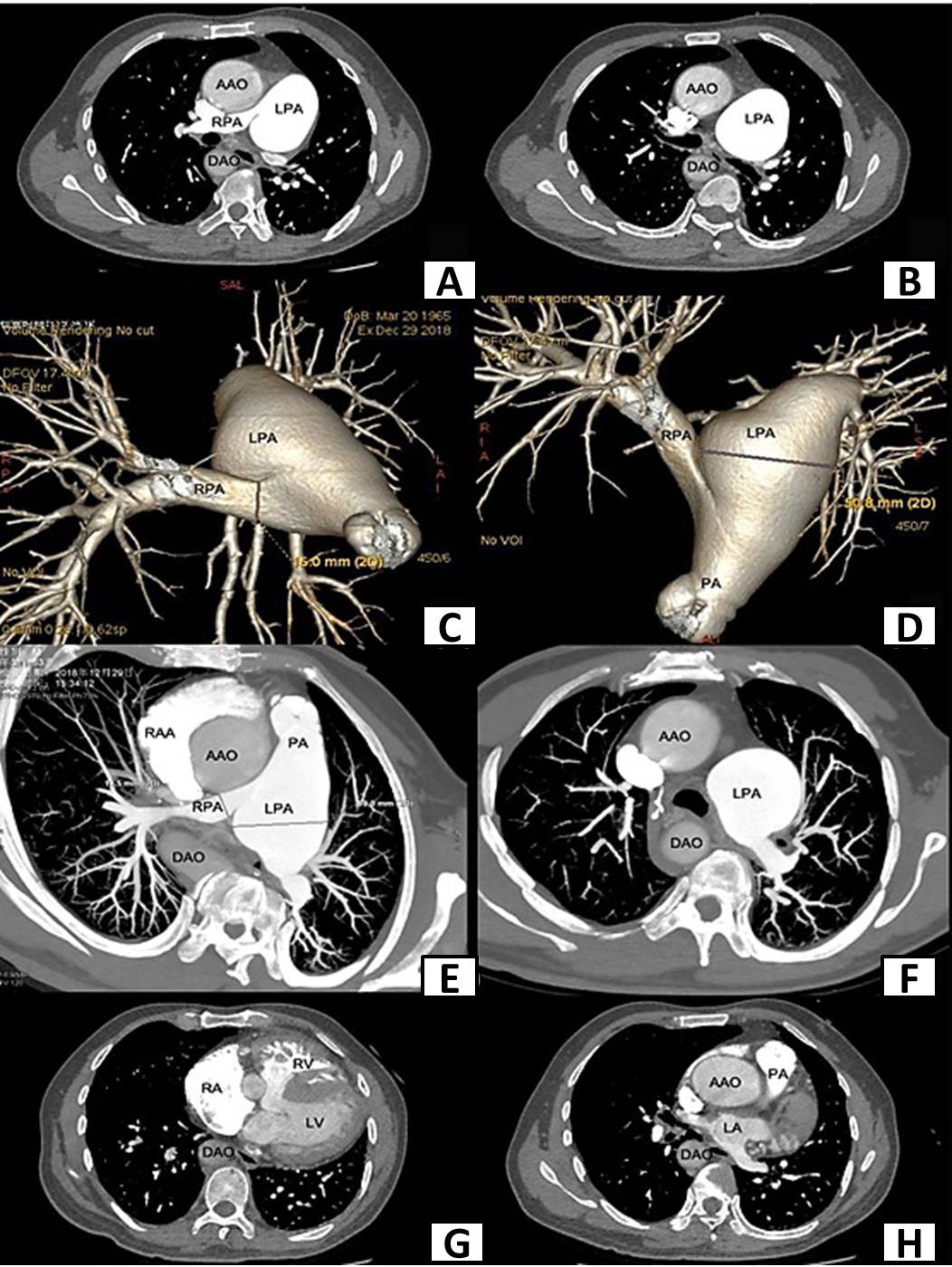
Enhanced cardiac computed tomography(CT) scan before surgery shows aortic overriding, ventricular septal defect, RVH and obstruction of right ventricular outflow tract (AAO, ascending aorta; DAO, descending aorta; LPA, left pulmonary artery; RPA, right pulmonary artery; PA, pulmonary artery; RAA, right atrial appendage; RA, right atrium; LA, left atrium; RV, right ventricle; LV, left ventricle). A, CT shows aortic override on the right pulmonary artery trunk and the dilated left pulmonary artery. B, CT shows dilated left pulmonary artery. C, CT shows stenosis of right pulmonary artery trunk and dilated left pulmonary. D, CT shows stenosis of right pulmonary artery trunk and dilated left pulmonary. E, CT shows aortic overriding, stenosis of right pulmonary artery trunk and dilated left pulmonary artery. F, CT shows dilated left pulmonary artery and thickened pulmonary branches. G, CT shows right ventricle hypertrophy and ventricular septal defect. H, CT shows aortic overriding and obstruction of right ventricular outflow tract.
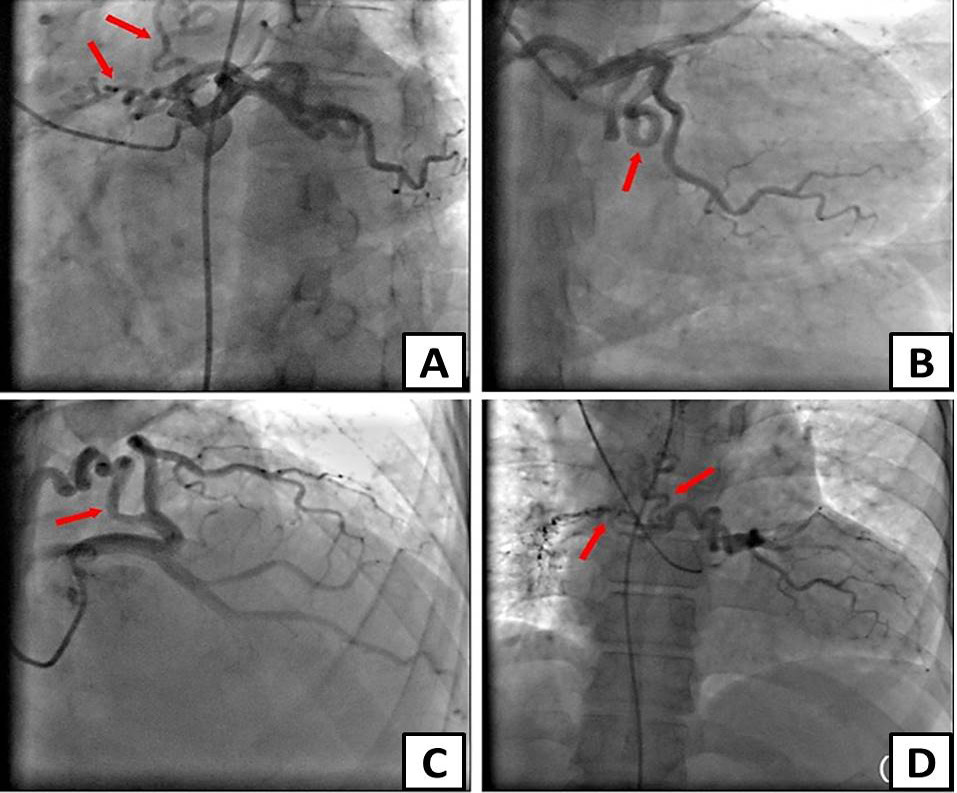
Selective coronary angiography shows a fistulous communication arising from the proximal left circum flex coronary artery to bronchial artery by different project positions. A, Coronary angiography in LAO45+CAU30 projection position. B, Coronary angiography in CAU20 projection position. C, Coronary angiography in RAO30+CRA30 projection position. D, Coronary angiography in AP projection position (red arrows show the fistulas).



{kind=link}
{kind=link}
{kind=link}