

Epidemiological and Clinical Correlates of Leukemia Ascertained in a Multiethnic Cohort of Pakistan




Epidemiological and Clinical Correlates of Leukemia Ascertained in a Multiethnic Cohort of Pakistan
Rehana Yasmin1,2, Rashda Abbasi2*, Tariq Saeed2, Madiha Sadiq2, Nuzhat Yasmeen3, Muhammad Iqbal4, A. Khuzaim Alzahrani5, Nadeem Kizilbash5, Ugur Bilge6, Nafees Ahmad2 and Sajid Malik1*
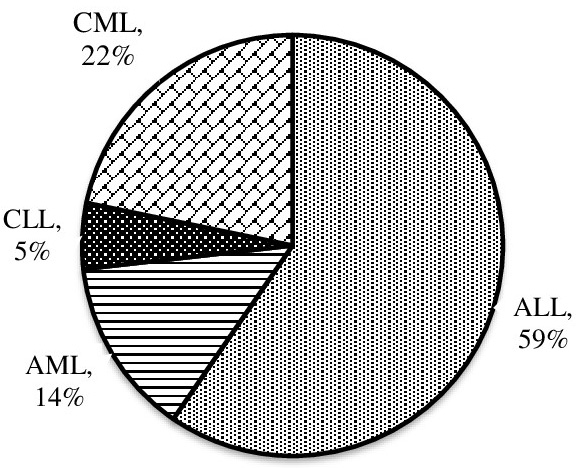
Percentage distribution of leukemia subtypes in Pakistani population, Acute lymphoblastic leukemia (ALL)was the most recurrent leukemia subtype, seen frequently in children (1-15 years). Myeloid leukemias (chronic myeloid leukemia; CML, acute myeloid leukemia; AML) were frequently seen in adults (15.1 – 39 and > 39 years), while chronic lymphocytic leukemia (CLL) was the least occurring leukemia subtype and observed only in adults (greater than 39 years old) in the study population.
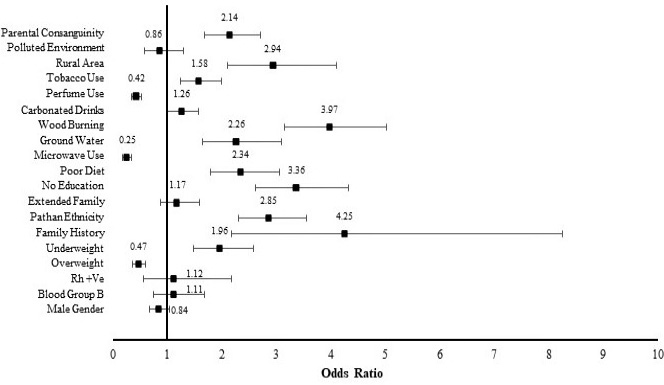
Odds ratios were calculated comparing the exposure of risk factor to patients and controls (CI 95%, p*= 0.05). It is indicated that lower BMI (ref. normal and higher BMI), poor diet (ref. standard BMI), all forms of tobacco use (ref. no use), consanguineous parental union (non-consanguineous parental union), family history of leukemia and solid cancers (ref. no family history), lack of basic education (ref. educated) and hailing to Pathan ethnicity (ref. other ethnicities additively) were high risks variables significantly associated to leukemia. In lifestyle related factors, wood burning, consumption of unprocessed ground water for drinking purposes, living in a residential rural set up were found to increase leukemia risk significantly and use of carbonated drinks was only observed to cause a slight but significant risk for leukemia; However, wearing perfume and microwave use has been observed to have protective effect for leukemia risk. The reference used for above factors were gas burning, water from all other sources, urban residential set up, no consumption of carbonated drinks, no use of perfume and no use of microwave, respectively. No significant risk-based association was noticed for extended family type, blood group B, Rh +ve, and gender in the studied population for leukemia patients in comparison to controls, taking nuclear family, all other blood groups than B, Rh -ve and female gender as reference.
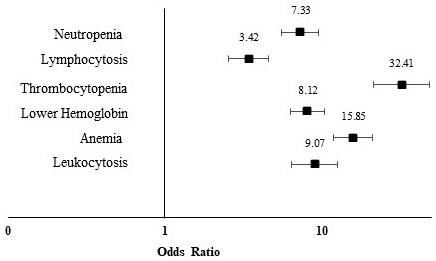
Leukocytosis (ref. additive model; normal count, leukocytopenia), lymphocytosis (ref. additive model; normal count, lymphocytopenia), are significantly associated to leukemia patients in comparison to age and gender matched controls (CI 95%, p* = 0.05). Also, on contrary, anemia (ref. additive model; normal count, erythrocytosis), hemoglobin (ref. additive model; normal and higher level), and thrombocytopenia (ref. additive model; normal count, thrombocytosis), were highly significant in leukemia patients.
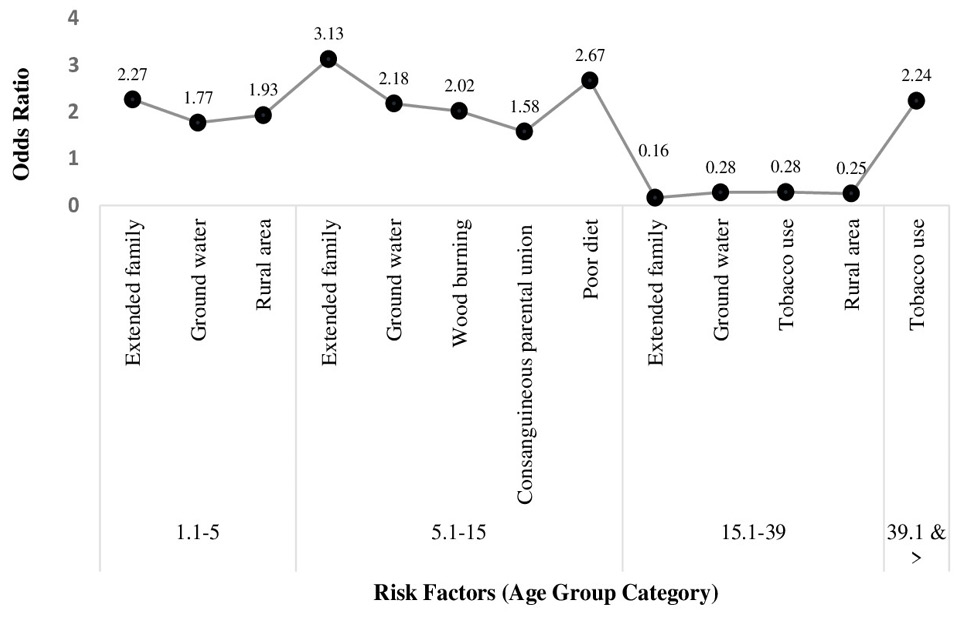
Odds ratios calculated to identify age group related risk factors for patients comparing to controls (CI 95%, p* = 0.05), indicated that although, extended family type was over all nonsignificant, but is a significant risk factor for children below age of 5 years with leukemia (ref. extended family type in remaining age groups), along with ground water consumption (ref. ground water consumption in all remaining age groups) and rural residential set up (ref. rural residential set up in remaining age groups). For patients of age 5.1-15 years old, extended family, ground water, wood burning (ref. wood burning in remaining age groups) as domestic fuel, consanguineous parental unions (ref. consanguineous parental unions in all remaining age groups), and poor diet (ref. poor diet in remaining age groups) were associated with high risk of leukemia. For patient older than 39 years of age, tobacco use (ref. tobacco use in remaining age groups) was significantly associated compared to controls; However, the for the Adolescents and young adults (AYAs; 15.1-39 years), designated as a unique group in oncology, although being a huge group in present study, the pattern was changed. As risk factors for other age groups, e.g., extended family, ground water, tobacco use, and rural residency are exhibiting protective effects when compared to age matched controls. The occurrence of the respective risk factor in all of the remaining age groups was treated as reference in each case.
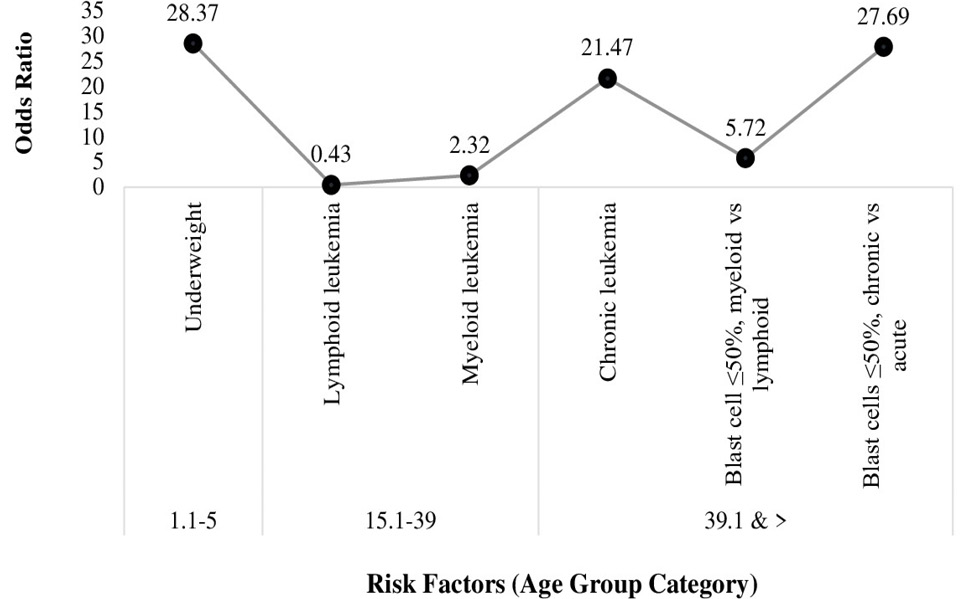
Odds ratios for identification of high-risk patients age group within the patient cohort (CI 95%, p* = 0.05), showed that among patients age groups, children (1.1-5 years) with lower BMI (ref. lower BMI in remaining age groups additively) were at higher risk for the disease. Patients in age group 15.1-39 have higher tendency to get myeloid leukemia (ref. myeloid leukemia in all other age groups additively) and in patients older than 39 years of age has higher risk for chronic leukemia (ref. chronic leukemia in remaining age groups additively). In patients older than 39 years old, the blast cells % for myeloid leukemia (ref. Blast cells ≤50% in myeloid leukemia in remaining age groups additively) and chronic leukemia (ref. Blast cells ≤50% chronic leukemia in remaining age groups additively) were significantly lower than lymphoid and acute in the same age groups, respectively.
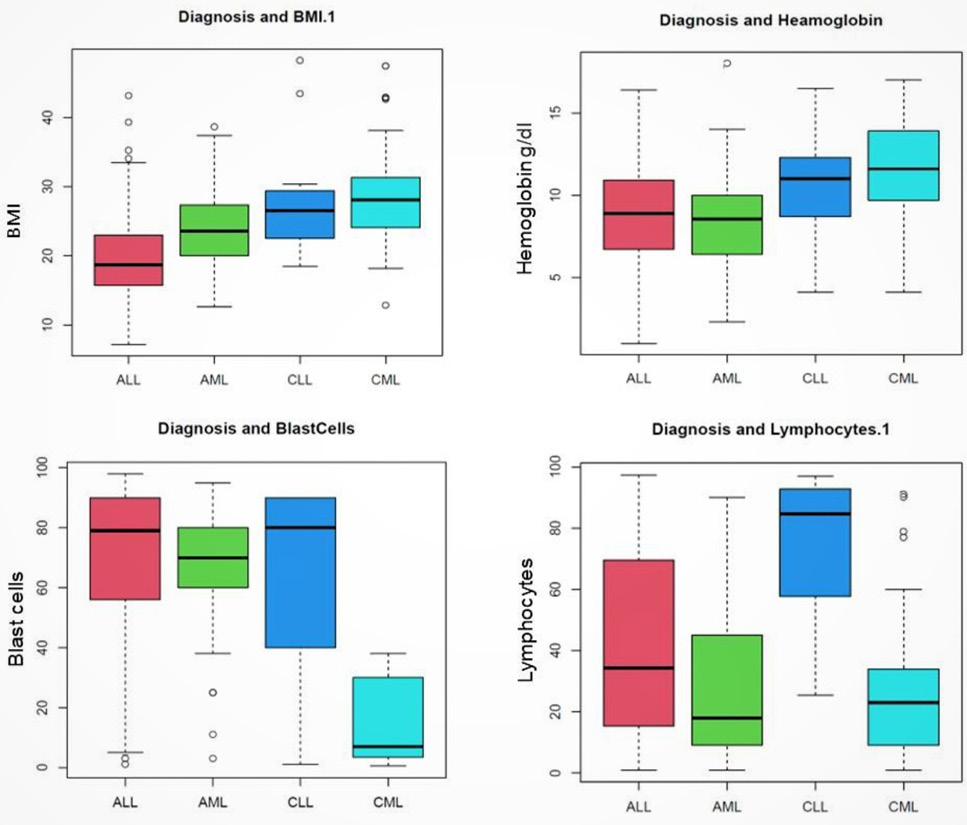
Patients with acute lymphoblastic leukemia (ALL), mostly comprised of children, presents lower BMI, higher count of blast cells and lower level of hemoglobin; patients with chronic myeloid leukemia (CML), majorly comprised of adults, have been observed to have higher BMI, lower percentage of blast cells, lower levels of lymphocytes and hemoglobin. Chronic lymphoid leukemia (CLL), comprised of adults of age greater than 39 years, showed the highest count of lymphocytes unlike any other subtype.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}