
South Asian Journal of Life Sciences


Research Article
South Asian Journal of Life Sciences 2 (2): 23 – 28Knowledge, Attitude and Practices towards Malaria: Union Council Bandagai Talash Dir (Lower), Pakistan
Haroon1, Atizaz Ahsan1, Ijaz Ahmad1, Tauseef Ahmad2*, Sikandar Khan Sherwani3, Rana Kausar4
- Department of Zoology, Shaheed Benaziar Bhutto University, Sherangal Khyber Pakhtunkhwa Pakistan
- Departments of Microbiology, Hazara University Mansehra, Khyber Pakhtunkhwa Pakistan
- Department of Microbiology, Federal Urdu University of Arts, Science and Technology Karachi, Pakistan
- Department of Microbiology, Federal Urdu University of Arts, Science and Technology Karachi, Pakistan
*Corresponding author:hamdardmicrobiologist@gmail.com
ARTICLE CITATION:
Haroon, Ahsan A, Ahmad I, Ahmad T, Sherwani SK (2014). Knowledge, attitude and practices towards malaria: union council bandagai talash dir (lower), pakistan. S. Asian J. Life Sci. 2 (2): 23 – 28.
Received: 2014–08–07, Revised: 2014–09–03, Accepted: 2014–09–23
The electronic version of this article is the complete one and can be found online at
(
http://dx.doi.org/10.14737/journal.sajls/2014/2.2.23.28
)
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
ABSTRACT
The present study was conducted in Union Council Bandagai Talash to assess the knowledge, attitude and practices (KAP) of learners on issues malaria. The aims of this survey is to collect information and aware the local population. This study was carried out in December 2013. The data was collected by a design questionnaire (standard and structured) for the knowledge, attitude and practice (KAP) study. Design questionnaire contain (sex, age, education, marital status, monthly income, occupation, symptoms, source of malaria, vector of malaria, curable and prevention measure) close and open ended question from Pato Talash, Khalisa Bajauro, Barikot, and Chinar Tangi. A total of 108 people were interviewed include 88 (81.48%) was males and 20 (18.52%) females aged between 0–>65 years. The level of education is not promising while fever, malaise and headache were reported the common symptom of malaria. From this survey it was concluded that the local population of Union Council Bandagai Talash have the basic knowledge about the malaria.
INTRODUCTION
On the surface of the globe malaria is still a major health problem especially for developing countries. Malaria caused 216 million cases and 655,000 deaths worldwide in 2010, of which 81% of the cases and 91% of the deaths were from sub–Saharan Africa (Abate et al., 2013). Worldwide each year more than 1 million peoples are died due to malaria and mostly the children (WHO, 2002).
Malaria is a mosquito borne disease cause by parasite known as plasmodium, which is transmitted by the bite of an infected Anopheles mosquito. The four species of plasmodium commonly infect humans known as plasmodium vivax, plasmodium falciparum, plasmodium malariae and plasmodium ovale. The P. vivax and P. falciparum are the most common species (Ahmad and Haroon, 2013). Symptoms include fever, vomiting, and headache and can appear 10 to 15 days after a bite. Prevention of the malaria through better understanding and awareness is the proper way to keep disease away and remain healthy. Use of insecticide–treated nets at home and indoor residual spraying with insecticides are recommended to reduce exposure to mosquito bites (Klein et al., 1995).
The situation was made more complicated by the rapid development, construction activities, unplanned rapid expansion of urban areas, industrialization without proper drainage facilities and development of supporting infrastructures like rail and roads without keeping in mind the natural flow of surface water (Dhaduk et al., 2013). Prevention and awareness is the appropriate way to keep disease away and remain healthy as illness confusion and health–seeking behavior may enhance or interfere with the effectiveness of control measures. Studies pertaining to knowledge, attitude and practices (KAP) showed that direct interaction with community plays an important role in circumventing malaria problem (Tyagi, et al., 2005). An understanding of the specific circumstances of each endemic zone with appropriate documentation could be used to modify the standard national malaria control program in order to reduce malaria incidence, and to prevent the emergence and spread of multi–drug resistant malaria, epidemic multi–drug resistant malaria threatens isolated communities and the wider population in a country facing many health and development challenge (Anh et al., 2005).
MATERIALS AND METHODS
The present study was conducted in Union Council Bandagai Talash to assess the knowledge, attitude and practices (KAP) of learners on issues malaria. The aims of this survey is to collect information and aware the local population. This study will be helpful to control malaria and also for any future prospect. It was a cross–sectional study conducted in Union Council Bandagai Talash Dir Lower, December 2013 during day time 9:00 AM to 12:00 PM. The data was collected from Pato Talash, Khalisa Bajauro, Barikot, and Chinar Tangi, by a design questionnaire (standard and structured) for the knowledge, attitude and practice (KAP) study. Design questionnaire contain (sex, age, education, marital status, monthly income, occupation, symptoms, source of malaria, vector of malaria, curable and prevention measure) close and open ended question. The local populations were interviewed randomly by on paper. The data were analyzed using Microsoft Excel 2007 version.
RESULTS AND DISCUSSION
In the current study a total of 108 peoples were interviewed for the KAP study on malaria in Union Council Bandagai Talash Dir Lower, during December 2013. The maximum 32 (29.63%) peoples were interviewed from Pato Talash, followed by Khalisa Bajauro 30 (27.78%), Barikot 30 (27.78%) and minimum people 16 (14.81%) from respondents were from Chinar Tangi (Figure 1).
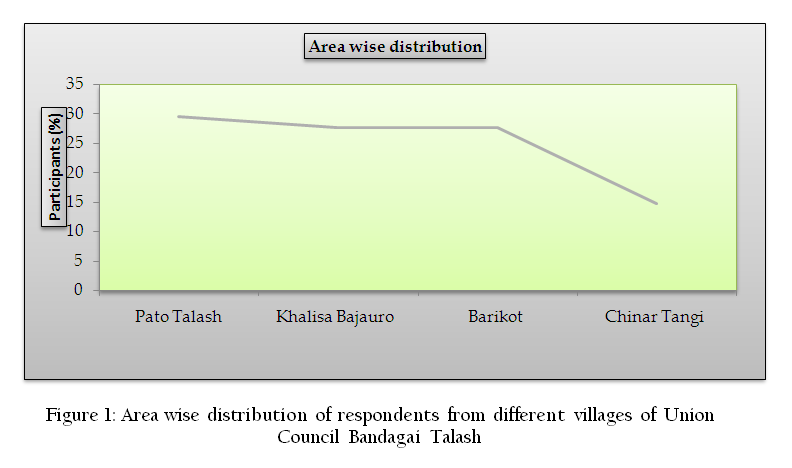
Figure 1: Area wise distribution of respondents from different villages of Union Council Bandagai Talash
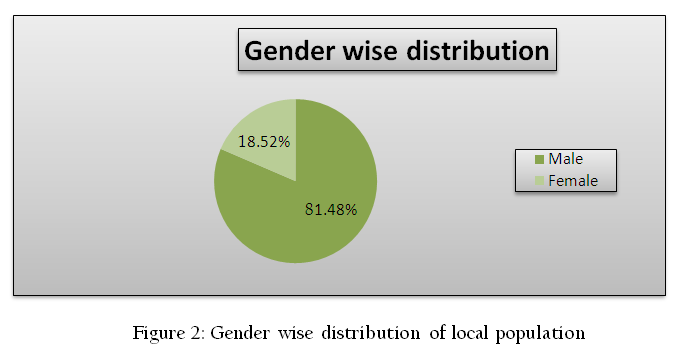
From total interviewed population 88 (81.48%) was males and 20 (18.52%) females as shown in Figure 2.
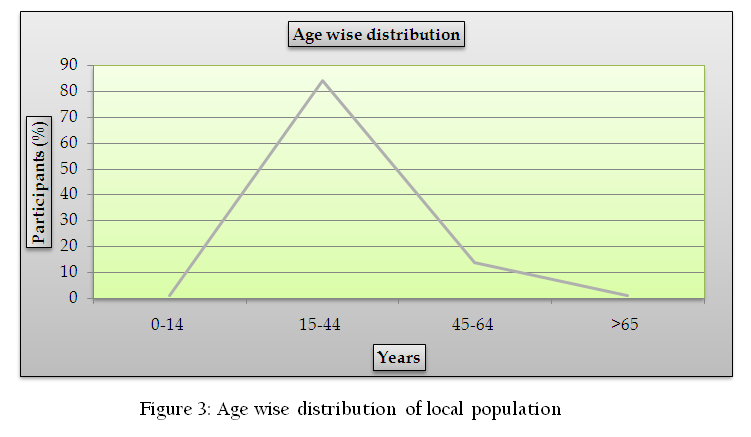
The population was interviewed by design questionnaire. Design questionnaire contain age, education, marital status, monthly income, occupation, symptoms, source of malaria, vector of malaria, curable and prevention measures. According to questionnaire the ages of local population are in different age groups the first group is 0–14 which has 1 (0.92%), second group 15–44 has 91 (84.26%), third group 45–64 has 15 (13.9%) and the fourth group >65 has 1 (0.92%) as shown in Figure 3.
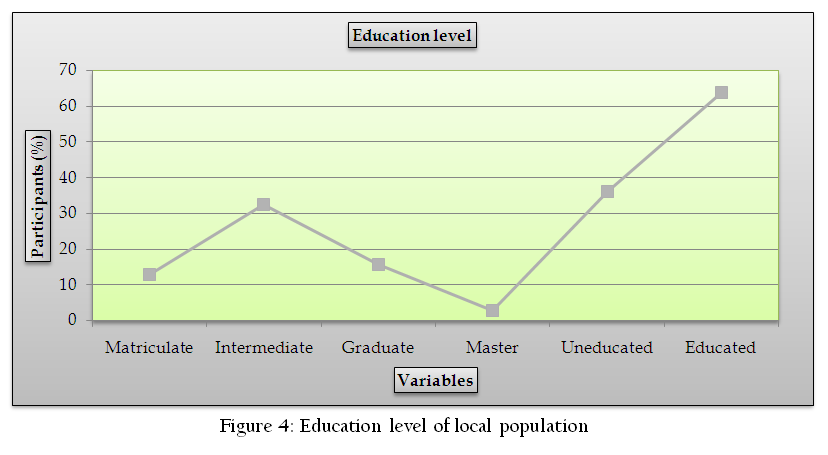
Our results shows that 69/108 (63.89%) population are educated while 39/108 (36.11%) uneducated. Out of the total educated population 14 (12.96%) are matriculate, 35 (32.41%) intermediate, 17 (15.74%) graduate and 3 (2.78%) master degree holder as shown in Figure 4. Our results is similar with findings of others reported high level of illiteracy (Ahmad et al., 2013; Ahmad and Haroon, 2013).
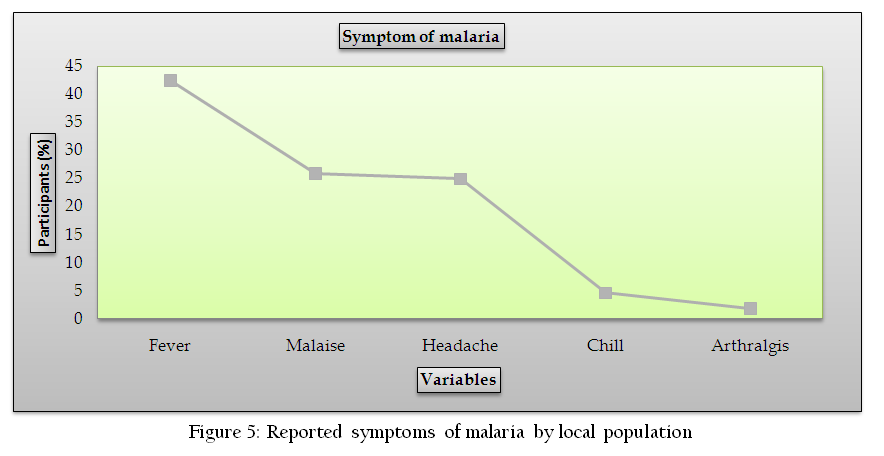
The current result shows that the local populations know about the symptoms of malaria 46 (42.59%) fever, 28 (25.93%) malaise, 27 (25%) headache, 5 (4.63%) chill and 2 (1.85%) arthralgis as shown in Figure 5. According to Ahmad and Hroon (2013) reported chill and fever are common symptoms of malaria in local population of Union Council Koaz Bahram Dheri, Pakistan.
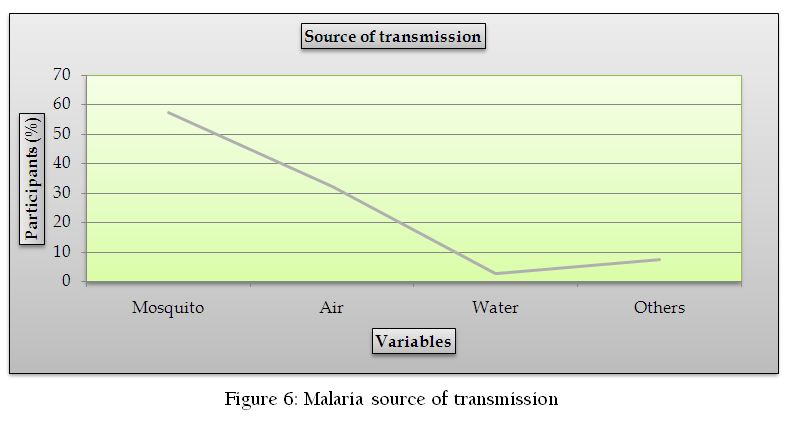
Local populations of Union Council Bandagai Talash represent good response against malarial transmission. Spreading of malaria from mosquito is 62 (57.41%), from air 35 (32.41%), water 3 (2.77%) and others 8 (7.41%) as shown in Figure 6. The results are in line with Ahmad and Haroon (2013) reported that mosquito is the common vector for the transmission.
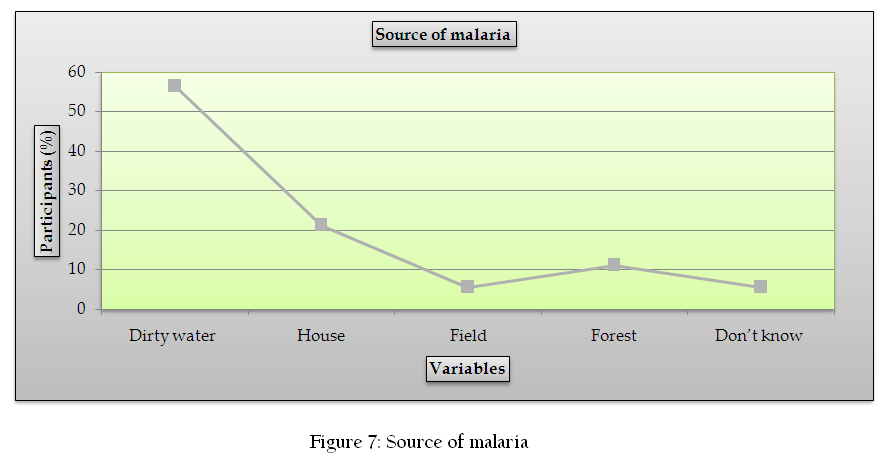
Malaria spread from dirty water 61 (56.58%) followed by house 23 (21.29%), field 6 (5.56%), forest 12 (11.11%) and don’t know 6 (5.56%) as shown in Figure 7.
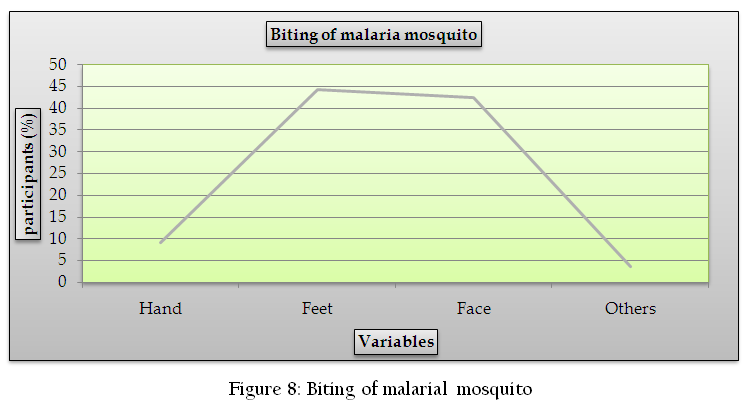
The local population was able to give answer about malarial mosquito where they bite. More views come about biting of face and feet. Hand 10 (9.26%), feet 48 (44.44%), face 46 (42.59%) and others 4 (3.7%) as shown in Figure 8.
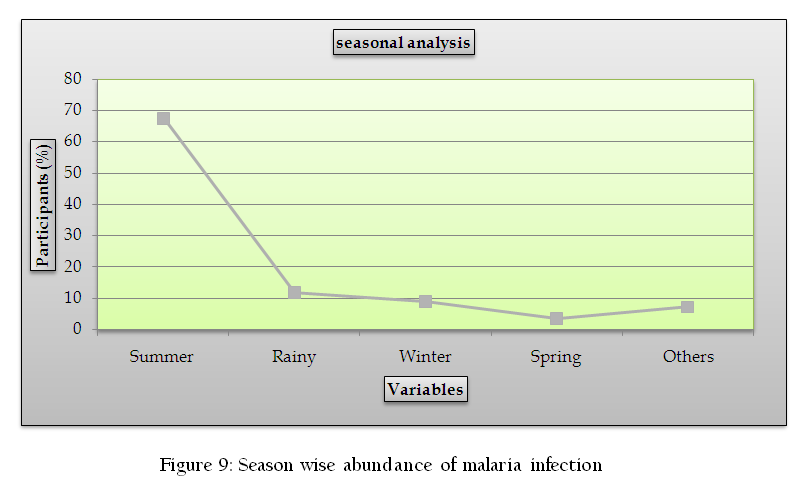
The season analysis shows that the malaria infection occurs mostly in summer season 73 (67.59%) followed by rainy season 13 (12.03%), winter season 10 (9.26%), others 8 (7.4%) and spring season 4 (3.71%) as shown in Figure 9. The result is similar with other (Ahmad and Haroon, 2013).
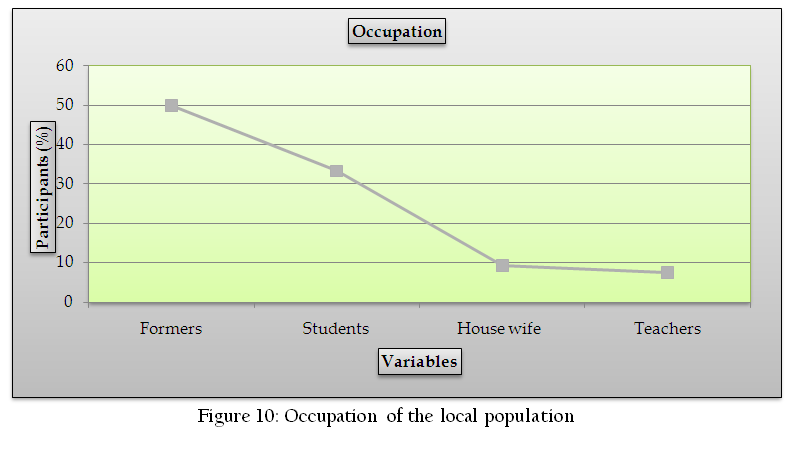
The local populations of the study area have a diverse occupation majority of them were formers 54 (50%) followed by students 36 (33.33%), House wife 10 (9.26%) and teachers 8 (7.41%) as shown in Figure 10.
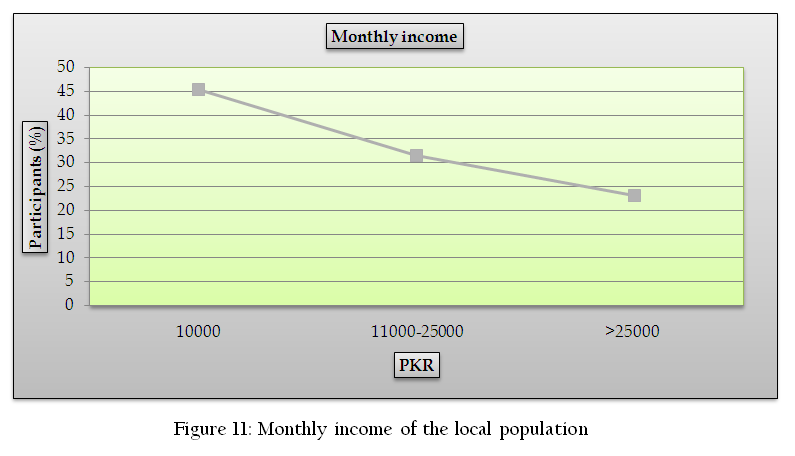
Socioeconomic condition of the local population were also considered which shows that the majority of peoples 49 (45.37%) have 10000 PKR monthly income followed by 11000–25000 PKR, 34 (31.48%) monthly income and those who have their monthly income is >25000 were 25 (23.15%) as shown in Figure 11.
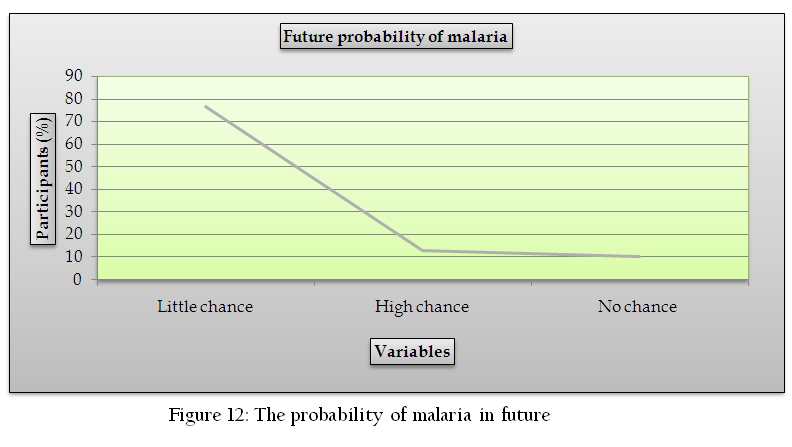
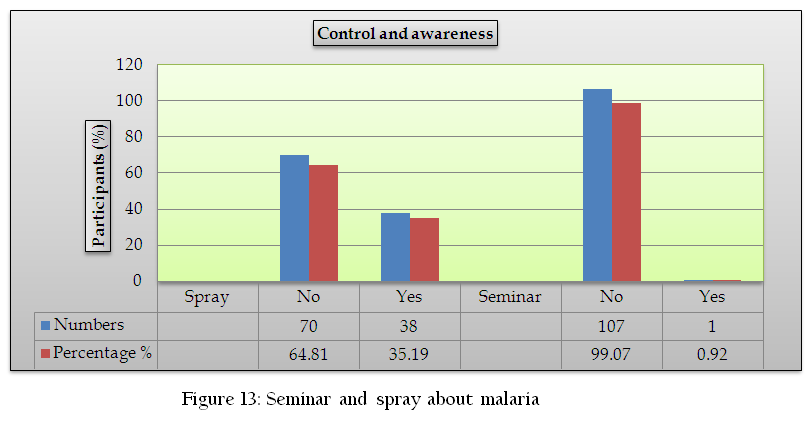
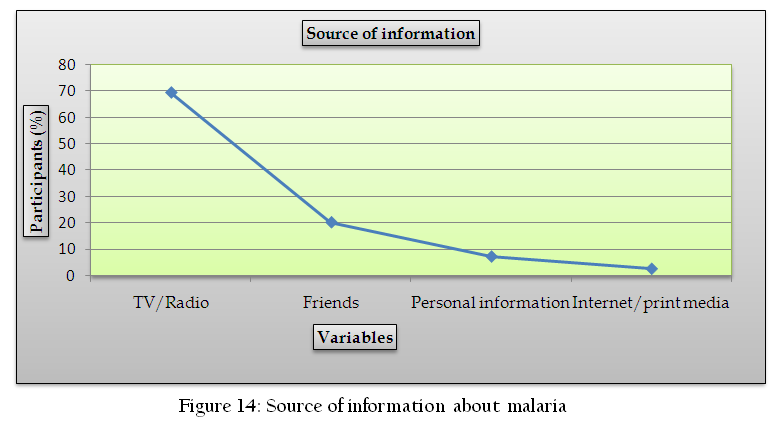
The majority of participants were respond that spreading of malaria have little chance 83 (76.85%) in future followed by high chance 14 (12.96%) and no chance 11 (10.19%) shown in Figure 12. According to local population if they adopt scientific methods, mosquito spray, mosquito net and others preventive measured they can stop malaria spreading. In Figure 13 describe, majority of participants answer that the government and non–government spray and not arrange any kind of awareness programs about malaria. Television and Radio 75 (69.44%) is the major source of information about malaria followed by friends 22 (20.37%), personal information 8 (7.41%) and internet/print media 3 (2.78%) as shown in Figure 14.
CONCLUSION
The local population of Union Council Bandagai Talash familiar with the symptoms of malaria, sources of mosquito, mode of transmission and also have general knowledge about the malaria. Rate of high illiteracy level and lack of awareness affect the control, elimination and eradication of any disease.
ACKNOWLEDGEMENT
We are very thankful to local population for their support. The conflict of interest was declared none.
REFERENCES
Abate A, Degarege A, Erko B (2013). Community knowledge, attitude and practice about malaria in a low endemic setting of Shewa Robit Town, northeastern Ethiopia. BMC P Health. 13: (312): 01 – 08.
Ahmad T, Haroon (2013). KAP study on Malaria in Union Council Koaz Bahram, Dheri, Pakistan. Asi J Nat & App Sci. 2(4): 30 – 37.
Ahmad T, Haroon M, Rahman SU (2013). Current Status of Education in Different Villages of Union Council Koaz Bahram Dheri, Pakistan. Eur Aced Res. 1(9): 2433 – 2437.
Anh NQ, Hung LX, Thuy HN, Tuy TQ, Caruana SR, Biggs BA, Morrow M (2005). KAP Surveys and Malaria Control in Vietnam: Findings and Cautions about Community Research. P. 572–577.
Dhaduk KM, Gandha KM, Vadera BN, Mehta JP, Parmar DV, Yadav SB (2013). A Community level KAP study on mosquito control in Jamnagar district. Natl J Com Med. 4(2): 321 – 328.
Klein RE, Weller SC, Zeissing R, Richards FO, Ruebush TK (1995). Knowledge, belief and practices in relation to malaria transmission and vector control in Guatemala. Am J Trop Med Hyg. 52: 383 – 8.
PMid:7771601
Tyagi P, Roy A, Malhotra MS (2005). Knowledge, awareness and practices towards malaria in communities of rural, semi–rural and bordering areas of east, Delhi (India). J Vect Borne Dis. 42, pp 30–35.
PMid:15999459
WHO (World Health Organization) Roll Back Malaria (2002). Malaria a global crisis. WHO Geneva Switzerland; Fact Sheet No. 1211.

