
Advances in Animal and Veterinary Sciences


Case Report

A Rare Case of Nasal Chondrosarcoma in a Dog
A. Arulmozhi**, S. Kathirvel*, B. Muralimanohar, R. Madheswaran, G.A. Balasubramaniam
*Department of Veterinary Surgery and Radiology, Veterinary College and Research Institute, Namakkal-2; Department of Veterinary Pathology, Veterinary College and Research Institute, Namakkal-2, India.
Abstract | This report deals about a rare case of nasal chondrosarcoma in a dog. A 10 years old male German shepherd dog was brought to the Teaching Veterinary Clinical Complex, Veterinary College and Research Institute, Namakkal with the history of progressive growth in the right nostril for the last 3 months. Clinically, there was a reddish pedunculated mass completely obliterating the right nasal passage and the tumour mass protruding through right nostril. Radiography of rostral view revealed a radio opaque mass in the right nostril. The fine needle aspiration and punch biopsy samples were collected for cytological and histopathological diagnosis respectively. In cytology, cluster of cells revealed pleomorphism, anisocytosis, anisokaryosis and mitotic figures were observed. Histopathologically, proliferating pleomorphic chondrocytes with increased mitotic activity and central area of necrosis were noticed. Sublingual lymphnodes sections also showed presence of pleomorphic chondrocytes. Surgical excision was not advised due to its extensive growth in the entire nasal passage, metastasis into sublingual lymphnodes and aggressive nature of tumour. The specific chemotherapy could not be undertaken due to lack of owner consent.
Keywords | Biopsy, Chondrocyte, Chondrosarcoma, Cytology, Histopathoogy
Editor | Kuldeep Dhama, Indian Veterinary Research Institute, Uttar Pradesh, India.
Received | August 25, 2017; Accepted | August 29, 2017; Published | October 26, 2017
*Correspondence | A. Arulmozhi, Department of Veterinary Surgery and Radiology, Veterinary College and Research Institute, Namakkal-2, India; Email: [email protected]
Citation | Arulmozhi A, Kathirvel S, Muralimanohar B, Madheswaran R, Balasubramaniam GA (2017). A rare case of nasal chondrosarcoma in a dog. Adv. Anim. Vet. Sci. 5(11): 460-462.
DOI | http://dx.doi.org/10.17582/journal.aavs/2017/5.11.460.462
ISSN (Online) | 2307-8316; ISSN (Print) | 2309-3331
Copyright © 2017 Arulmozhi et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Introduction
Chondrosarcoma of the bone is a fast spreading and malignant form of cancer and if it is not diagnosed and treated early, can be life threatening (Vasanth, 2016). Primary chondrosarcomas are malignant, slow growing and locally invasive tumours of skeletal and extra skeletal cartilage (Cohen et al., 2010). It is the second most common primary bone tumour in both human and dogs and it accounts for approximately 5% to 10% of all canine primary bone tumours (Straw, 1996). The large breed dogs are most frequently affected (Ling et al., 1974). Different types of chondrosarcoma have been described as conventional chondrosarcoma (90% of all chondrosarcomas), dedifferentiated chondrosarcoma, clear cell chondrosarcoma, mesenchymal chondrosarcoma, juxtacortical chondrosarcoma and secondary chondrosarcoma (Murphey et al., 2003). The major sites of chondrosarcomas were the ribs (29%), nasal cavity (26%) and pelvis (Brodey et al., 1974). Nasal and paranasal sinus tumors account for only 1-2% of all canine tumors and 21 % of tumours in nasal and paranasal regions of dogs were chondrosarcoma (Brown et al., 2015). There is no published report from Tamil Nadu and India on chondrosarcomas in the nasal and paranasal regions of dogs. The present report deals about a rare case of nasal chondrosarcoma in a dog.
Materials and methods
A male 10 years old German shepherd dog was brought to the Teaching Veterinary Clinical Complex, Veterinary College and Research Institute, Namakkal with the history of progressive growth in the right nostril for the last 3 months. The dog was clinically examined and blood and serum sample were collected for routine haemogram and serum biochemistry. Radiography was taken to ascertain the extent of the growth and metastasis. A Fine needle aspiration biopsy was collected from the nasal growth for cytological studies. The impression smears from tissue biopsy were stained with Ziehl-Neelsen, Grams and lactophenol cotton blue stain to screen the acid-fast organisms, bacterial and fungal etiology respectively. Punch biopsy samples from nasal and sublingual lymphnodes were preserved in 10% formalin for histopathological examination. The processed tissue specimens were embedded in paraffin and section were cut at 5 micron thickness. The paraffin sections were deparaffinized by using xylene I and II (2 minutes each). Hydration of the tissue sections were made by passing through decreasing concentration of alcohol and water (100%, 90%, 80%,70%) and they were stained with hematoxylin for 5 minutes. Then they were washed in running tap water until the sections becomes “blue” and stain with 1% Eosin Y for 10 minutes. Wash in tap water for 1-5 minutes. Dehydrate the sections in increasing concentration of alcohols and clear in xylene (Bancroft and Stevens, 1996).
Results and Discussion
Clinically, there was a reddish pedunculated mass completely obliterating the right nasal passage and the tumour mass protruding through right nostril (Figure 1). Thick mucus discharge from the left nostril, tachypnea, snoring, halitosis, disfigurement of face, epiphora and enlargement of sublingual lymph nodes were noticed.

Figure 1: Reddish pedunculated mass completely obliterating the right nasal passage and protruding through right nostril
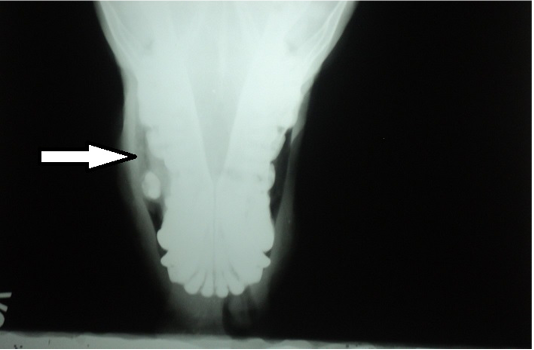
Haemogram revealed normal haematological values viz. Haemoglobin - 14 .8 g/dl, PCV- 42%, RBC count – 7.2 x 106/ cu.mm and WBC count -6x103/cu.mm. Likewise, differential leucocyte count and serum biochemical values were also within the normal range. Radiography of rostral view exhibited a radio opaque mass (arrow) in the right nostril (Figure 2). In cytology, cluster of cells (Figure 3) revealed pleomorphism, anisocytosis, anisokaryosis and mitotic figures. Tissue impression smears did not reveal either acid-fast bacilli / other bacteria or fungal organisms.

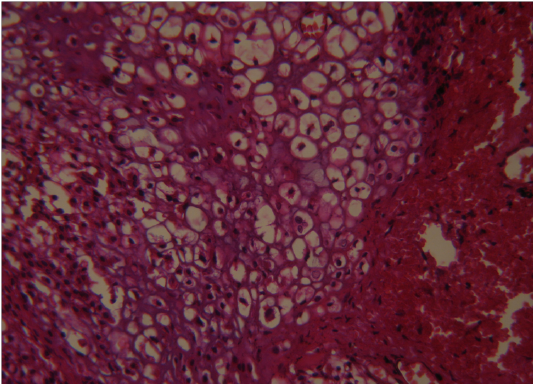
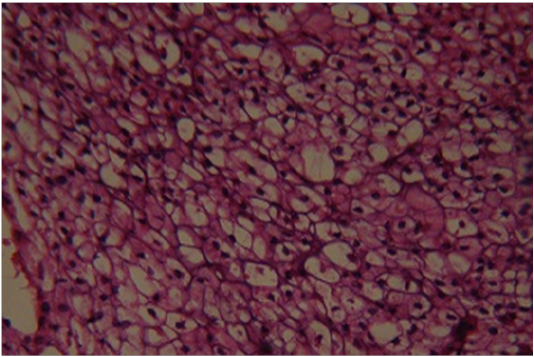
Histopathologically, proliferating neoplastic cells seen among the fibrous tissue. There were severe necrotic changes in the tumour mass under mucosal epithelium and also submucosal haemorrhage due to expanding tumour mass. The tumour mass showed the pleomorphic chondrocytes with numerous mitotic figures (Figure 4). Proliferating pleomorphic chondrocytes with increased mitotic activity and central area of necrosis suggestive of a high-grade chondrosarcoma. Formation of necrotic core at the centre of the mass might be due to the newly proliferating cells pushed towards its centre and resulted in deprivation of vital nutrients. Sublingual lymphnodes also revealed pleomorphic chondrocytes (Figure 5) which has exemplified the metastatic nature of the tumour. Similarly, metastasis of chondrosarcoma in renal tissues was also recorded by Hahn et al. (1997).
Surgical resection was not advised due to its extensive growth in the entire nasal passage, metastasis into sublingual lymphnodes and aggressive type in histologic picture. The histomorphology picture revealed the presence of clear cell chondrocytes which had the abundant vacuolated cytoplasm due to the presence of glycogen (Murphey et al., 2003). Hence, this case was confirmed as clear cell chondrosarcoma.
Earlier authors also recorded the recurrence and metastasis of chondrosarcoma even after its surgical resection (Suzanne et al., 2007). The specific chemotherapy could not also be undertaken due to lack of owner consent.
Conflict of interest
There is no conflict of interest.
AUthors Contribution
All authors contributed equally.
References

