Research Journal for Veterinary Practitioners


Case Report
Research Journal for Veterinary Practitioners 2 (3): 49 – 51Removal of Oesophageal Foreign Body by Transthoracic Oesophagotomy in a Tibetan spaniel Dog
Musa Korkmaz1*, Kamuran Pamuk1, Basak Tuncer Ulukartal2
- Department of Surgery, Faculty of Veterinary Medicine, Afyon Kocatepe University, 03200, Afyonkarahisar, Turkey
- Cat&Dog Veterinary Policlinic, Izmir, Turkey
*Corresponding author:musakorkmaz@aku.edu.tr
ARTICLE CITATION:
Korkmaz M, Pamuk K and Ulukartal BT (2014). Removal of oesophageal foreign body by transthoracic oesophagotomy in a Tibetan spaniel dog. Res. J. Vet. Pract. 2 (3): 49 – 51.
Received: 2014–02–10, Revised: 2014–02–27, Accepted: 2014–02–28
The electronic version of this article is the complete one and can be found online at
(
http://dx.doi.org/10.14737/journal.rjvp/2014/2.3.49.51
)
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
ABSTRACT
This report describes removal of an oesophageal foreign body by transthoracic oesophagotomy in a Tibetan spaniel dog. An 8 year–old, weighing 4 kg, male Tibetan spaniel dog was referred with complaint of regurgitation, vomiting and weight loss. In clinical examination, regurgitation, dysphagia, hyper–salivation, abdominal respiration, cough and depression were observed. In thoracic radiography, presence of an irregular–shaped radiopaque foreign body was detected between heart and diaphragm in thoracic part of oesophagus. Oesophageal foreign body was removed by transthoracic oesophagotomy. After thoracotomy, a gastrostomy tube was placed in the stomach of animal and it was hospitalized for one week and it was fed by this way. The control examination at the end of hospitalization period showed that the dog could take liquids orally and recovery was completely achieved.
Oesophageal foreign bodies are a common clinical disorder which can become life threatening in dogs (Speilman et al., 1992; Kyles, 2003; Sale and Williams, 2006). The frequently encountered oesophageal foreign bodies are bones and bone fragments in dogs. Moreover, fishhooks, rawhide, wooden sticks, balls, chew treats toys, pieces of plastic or metal and other varied objects have been also reported (Speilman et al., 1992; Luthi, 1998; Moore, 2001; Sale and Williams, 2006; Rousseau et al., 2007; Thompson et al., 2012).
Common clinical signs associated with oesophageal foreign bodies are regurgitation or vomiting, retching, gagging, lethargy, anorexia, restlessness, distress, ptyalism and cough (Moore, 2001; Sale and Williams, 2006; Leib and Sartor, 2008; Juvet et al., 2010; Thompson et al., 2012). The severity of the clinical signs depends on size, type and location of the foreign bodies, and the duration of obstruction, presence or absence of a stricture or a wall perforation, pneumothorax, pleuritis, pneumomediastinum, hemothorax and/or pyothorax (Gienella et al., 2009).
It has been reported that foreign bodies may be seen any part oesophagus, but the presence of the anatomically narrowed regions of oesophagus is the most predisposing factor for the occurrence of these bodies. These regions are known as pharyngeal oesophagus, thoracic inlet, base of the heart and distal oesophagus (Houlton et al., 1985). The most commonly noticed location is the caudal oesophagus between the heart base and diaphragm (Moore, 2001; Sale and Williams, 2006; Leib and Sartor, 2008; Thompson et al., 2012).
This report describes clinical and radiographic findings and removal of the oesophageal foreign body by transthoracic oesophagotomy in a Tibetan spaniel dog.
An 8–year–old, male Tibetan spaniel dog, weighing 4 kg was referred with complaint of regurgitation, vomiting and weight loss. The owner noted that the dog was fed by sheep bones about four months ago and then, dysphagia, gagging and retching were observed. Moreover, the owner also stated that unlike liquid foods, vomiting was evident after eating the solid foods. In clinical examination, regurgitation, dysphagia, hypersalivation, abdominal respiration, cough and depression were observed. Moreover, incoordination in the back feet was detected. In thoracic radiography, presence of an irregular–shaped radiopaque foreign body was detected between heart and diaphragm in thoracic part of oesophagus (Figure 1) and it was thought that it could be a solid foreign body, i.e. bone fragment. Since the irregular shape of foreign body, surgical removal was performed instead of endoscopical approach due to possible perforation risk of oesophagus.
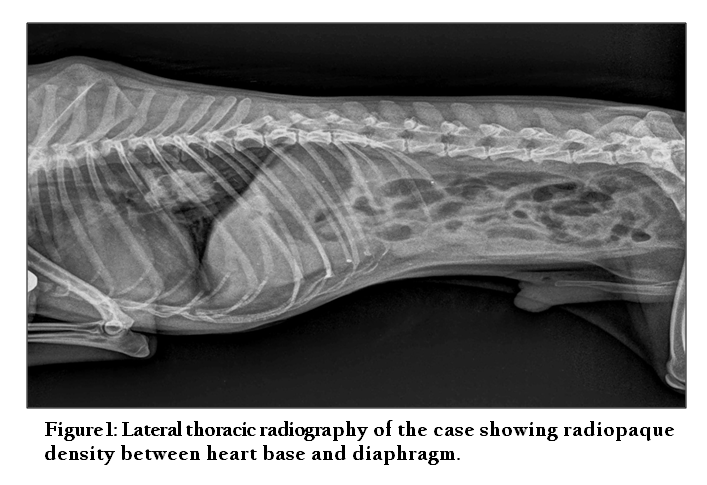
Figure 1: Lateral thoracic radiography of the case showing radiopaque density between heart base and diaphragm
The dog was administered 0.04 mg/kg atropine sulphate (Atropine, Vetas, Turkey) subcutaneously 30 min before the surgery. The dog was premedicated with 0.3 mg/kg midazolam (Dormicum, Roche, Turkey) given intravenously. Induction of anaesthesia was performed with 6 mg/kg propofol (Propofol, Abbott, Turkey) via IV bolus. Following endotracheal intubation, general anaesthesia was maintained at 2% isoflurane (Forane, Abbott, Turkey). Cephalic vein was cannulated for the administration of lactated Ringer’s solution (10 mL/kg/h) during the surgical procedure.
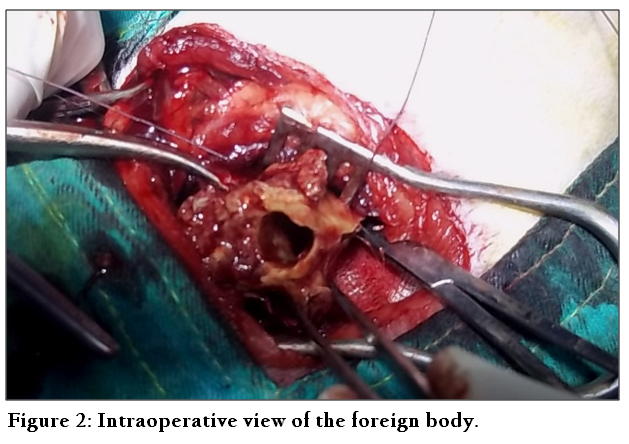
The dog was positioned in right lateral recumbency, and a standard left intercostal thoracotomy was performed. The oesophagus was identified, and branches of the vagus nerve were gently retracted from the affected site. Non–absorbable sutures were placed on both sides of the oesophageal incision site to provide traction and stability during oesophageal manipulation. Saline–soaked sponges were packed around the proposed incision site to limit contamination of the pleura. A dorsal or left lateral longitudinal incision was made in the oesophagus overlying the foreign body. The foreign body (sheep vertebral bone) (Figure 2) was grasped and removed by gentle manipulation and traction. The mucosal surface of the oesophageal wall was debrided as necessary and was closed using a double–layer technique with 2/0 polyglactin 910 (Vycrl, Eticon, UK). Thoracotomy tube was then inserted through the thoracic wall. The thoracotomy was closed routinely. Air and fluid were drained from the pleural cavity via the thoracotomy tube immediately after closure. Thoracotomy tube was removed immediately after anaesthesia if an effusion was not present.
After thoracotomy, a gastrostomy tube was placed in the stomach of animal and it was hospitalized for one week and it was fed by this way. During postoperative 7 days cefazolin sodium 22 mg/kg (Sefazol, Mustafa Nevzat Ilac Sanayi, Turkey) was applied intramuscularly. After 1 week control of the dog it was observed that the dog could take liquids orally and gastrostomy tube was removed.
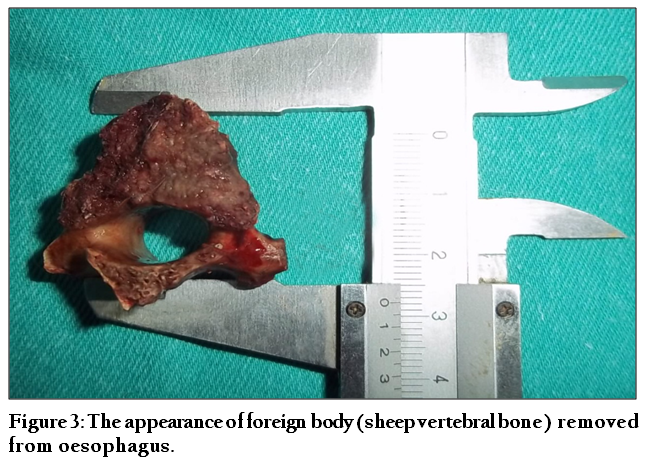
During oesophagotomy, it was seen that the foreign body was an irregular shaped sheep vertebral bone (2x2.5 cm) (Figure 3). Moreover, it was observed that the position of this irregular shaped sheep vertebral bone provided the partially food transition from its vertebral channel. Therefore, this unexpected condition may explain how the animal could be survived for four months without any therapy. In radiography of oesophagus taken after one week, no leakage was observed from the surgical wound and no complication was occurred related to oesophagus.
It has been reported that the localization of oesophageal foreign bodies in dogs is mostly thorax entrance or thoracic area (Moore, 2001; Sale and Williams, 2006; Leib and Sartor, 2008; Thompson et al., 2012) and common observed oesophageal foreign bodies are bone or bone fractures (Moore, 2001; Sale and Williams, 2006; Rousseau et al., 2007). Moreover, chew treats, balls, toys, fish pole and metal, plastic or wood pieces have also been noted in dogs (Speilman et al., 1992; Luthi, 1998; Moore, 2001; Sale and Williams, 2006; Rousseau et al., 2007; Thompson et al., 2012). In this case, foreign body that was removed from oesophagus was a sheep vertebral bone which was located between heart and diaphragm in accordance with previous reports (Sale and Williams, 2006). It was observed that bone had a considerable irregular surface with sharp edge. Interestingly, food transition was partially provided from vertebral channel that existed in the middle of the bone. Therefore, the animal could survive for four months without any therapy.
Oesophageal foreign bodies have been mostly reported in small breed dogs (Moore 2001; Sale and Williams, 2006; Rousseau et al., 2007; Leib and Sartor., 2008; Gienella et al., 2009; Thompson et al., 2012). In many studies, the common dog breeds predisposing to oesophageal bodies are Yorkshire Terrier, West Highland Terrier, Shih Tzu (Rousseau et al., 2007; Leib and Sartor, 2008; Gienella et al., 2009; Juvet et al., 2010) Maltese Terrier, Shetland Sheepdog (Leib and Sartor, 2008; Thompson et al., 2012). On the other hand, Golden Retriever, Labrador Retriever (Gienella et al., 2009), German Shepherd Dog, Beagle, Eskimo, English Bulldog, Chow Chow, Pug (Thompson et al., 2012), Bull Mastiff, Boxer (Sale and Williams, 2006) dogs suffering from oesophageal foreign body have been also reported. In this study, oesophageal foreign body obstructed in a small breed dog such as Tibetan spaniel was consistent with the above–mentioned reports. Furthermore, this report is the first, to describe the surgical treatment of oesophageal foreign body in a Tibetan spaniel in our clinics.
Mostly seen clinical symptom in dogs having oesophageal foreign body is regurgitation following feeding (Speilman et al., 1992; Moore, 2001; Sale and Williams, 2006; Leib and Sartor, 2008; Thompson et al., 2012). It has been indicated that clinical symptoms such as regurgitation, gagging and retching following feeding are important observations associated with pharyngeal occlusion, oesophagitis, oesophageal foreign objects, neoplasia, vascular ring anomaly, perioesophageal masses, granulomas, megaloesophagus, oesophageal diverticulum and hiatal diseases (Willard and Weyrauch, 1999). In this case, primer clinical symptom was regurgitation. However, vomiting, gagging and coughing were observed. It has been well documented that direct and indirect radiography should be applied, if the regurgitation is evident. In the presented case, the thoracic radiography showed the presence of foreign body which localized between heart base and diaphragm. The process of diagnosis was consistent with Willard and Weyrauch (1999) and it is suggested that direct and indirect thorax radiography is a basic tool to diagnose oesophageal foreign bodies following the clinical symptoms such as regurgitation, vomiting, retching and gagging.
Endoscopy is commonly used for removal of oesophageal foreign bodies in dogs (Moore, 2001; Rousseau et al., 2007; Leib and Sartor, 2008; Gianella et al., 2009; Juvet et al., 2010; Keir et al., 2010; Thompson et al., 2012). Pushing oesophageal foreign bodies localized at thoracic area towards stomach by using rigid catheter or removing foreign body with gastrostomy are possible treatment options (Leib and Sartor, 2008; Gianella et al., 2009; Juvet et al., 2010; Thompson et al., 2012). Moore (2001) has reported that oesophageal foreign bodies could be removed orally with guidance of fluoroscopy and the help of forceps. Moreover, it has been suggested that transthoracic oesophagotomy is the best choice in the cases which the foreign body is not possible to remove by endoscopy (Sale and Williams, 2006). In the presented case, the bone was removed by surgery instead of endoscopical approach due to possible perforation risk of oesophagus, since the irregular shape of foreign body. It is suggested that transthoracic oesophagotomy is the best approach when the surgeon presumed that the foreign body has an irregular shape in nature.
It has been postulated that the application transthoracic oesophagotomy has some complications such as pyothorax, mediastinitis, pleural effusion (Sale and Williams, 2006), hydrothorax, pleuritis and continued non–healing wound or gall duct (Speilman et al., 1992; Kyles, 2003). In this case, after the surgery, the dog was feed for one week by placing gastrostomy tube in the stomach of the dog. Oesophagus radiographies showed that no gall duct or dehiscence on the operation wound was evident end of the first week after surgery. It was observed that approximately ten days later, the animal had clinically good health and body condition without any postoperative complication.
In conclusion, this unique case describes the successful treatment of oesophageal foreign body existed for four months. It is suggested that transthoracic oesophagotomy can be applied successfully for removing oesophageal foreign bodies which is not possible to remove by using endoscopy or fluoroscopic method at thoracic area in dogs.
REFERENCES
Gianella P, Pfammatter NS and Burgener IA (2009). Oesophageal and gastric endoscopic foreign body removal: complications and follow–up of 102 dogs. J Small Anim Pract, 50: 649–54.
http://dx.doi.org/10.1111/j.1748-5827.2009.00845.x
PMid:19954441
Houlton, J.E.F., Herrtage, M.E., Taylor, P.M. and Watkins, S.B. 1985. Thoracic esophageal foreign bodies in the dog: a review of ninety cases. J Small Anim Pract, 26: 521–536.
http://dx.doi.org/10.1111/j.1748-5827.1985.tb02230.x
Juvet, F., Pinilla, M., Shiel, R.E. and Mooney., C.T. 2010. Oesophageal foreign bodies in dogs: factors affecting success of endoscopic retrieval. Ir Vet J, 63, 163–8.
http://dx.doi.org/10.1186/2046-0481-63-3-163
PMid:21851744 PMCid:PMC3113842
Keir, I., Woolford, L., Hirst, C. And Adamantos S. 2010. Fatal aortic oesophageal fistula following oesophageal foreign body removal in a dog. J Small Anim Pract, 51: 657–60
http://dx.doi.org/10.1111/j.1748-5827.2010.01012.x
PMid:21121922
Kyles, A.E. 2003. Surgical diseases of the esophagus, In: Slatter, D. (editor), 3rd ed. Textbook of Small Animal Surgery, WB Saunders, Philadelphia, pp: 573–591.
Leib, M.S. and Sartor L.L. 2008. Esophageal foreign body obstruction caused by a dental chew treat in 31 dogs (2000–2006). J Am Vet Med Assoc, 232: 1021–5.
http://dx.doi.org/10.2460/javma.232.7.1021
PMid:18380620
Luthi, C. 1998. Esophageal foreign bodies in dogs: 51 cases (1992–1997). Eur J Comp Gastroenterol, 3: 7–11.
Moore, A.H. 2001. Removal of esophageal foreign bodies in dogs: use of the fluoroscopic method and outcome. J Small Anim Pract, 42: 227–230.
http://dx.doi.org/10.1111/j.1748-5827.2001.tb02025.x
PMid:11380014
Rousseau, A., Prittie, J., Broussard, J.D., Fox, P.R., and Hoskinson J. 2007. Incidence and characterization of esophagitis following esophageal foreign body removal in dogs: 60 cases (1999–2003). J Vet Emerg Crit Care, 17: 159–163.
http://dx.doi.org/10.1111/j.1476-4431.2007.00227.x
Sale, C.S.H. and Williams, J.M. 2006. Results of transthoracic esophagostomy retrieval of esophageal foreign body obstruction in dogs: 14 cases (2000–2004). J Am Anim Hosp Assoc, 42: 450–456.
PMid:17088392
Spielman, B.L., Shaker, E.H. and Garvey, M. 1992. Esophageal foreign body in dogs: a retrospective study of 23 cases. J Am Anim Hosp Assoc, 28: 570–574.
Thompson, H.C., Cortes, Y., Gannon, K., Bailey, D. and Feer, S. 2012. Esophageal foreign bodies in dogs: 34 cases (2004–2009). Journal of Vet Emerg and Crit Care, 22: 253–261.
http://dx.doi.org/10.1111/j.1476-4431.2011.00700.x
PMid:23016814
Willard, M.D. and Weyrauch E.A. 1999. Esophagitis, In: Kirk, R.W. and Banoguno, J. (editör), 13th edition, Kirk's Current Veterinary Therapy–Small animal practice, WB Saunders, Philadelphia, pp: 607–610.