
Advances in Animal and Veterinary Sciences


Research Article

A Cross Sectional Study to Understanding Demographics of Dog Bite Victims Attending Anti Rabies Ward in Chennai City, Tamil Nadu India
Sukumar Bharathy*, Lakshmanasami Gunaseelan
Department of Veterinary Public Health and Epidemiology, Madras Veterinary College, Chennai- 600 007.
Abstract | This cross sectional study was conducted by interviewing people attending the anti- rabies ward for post exposure rabies vaccination in a three Government General Hospitals, Chennai city. A total of 256 victims of dog bites from different areas of Chennai were interviewed with a pre tested structured questionnaire after informed verbal consent from victims between April 2013 and April 2014. Out of total 256 victims of dog bite, majority were males (71.87%) in the age group of 11 to 20 years (21.49%). Students outnumbered the general population (33.97%). Higher number of victims of dog bites was reported from Central Chennai. While 46 per cent of victims were bitten by stray dogs,in majority of victims, bite wounds were found in lower portion of the body (59.77%) with major exposure being minor scratches (57.4%). Fifty one per cent of bite victims washed their wounds and 48.44 per cent attended antirabies ward within 24 hours for post exposure prophylaxis. Our findings highlighted that a larger proportion of the bites were provoked, from owned pet dogs with exposures being very minor (scratch) in majority of cases which may not need post bite immunization. There is an urgent need to focus the educational campaigns throughout Chennai city with an effective dog population management combined with strategic immunization program and the effective use of rabies RIG and vaccination in dog bite cases as warranted could help to reduce rabies deaths.
Keywords | Bites victims, Human rabies, Post bite immunization, Risk factors.
Editor | Kuldeep Dhama, Indian Veterinary Research Institute, Uttar Pradesh, India.
Received | November 20, 2016; Accepted | February 16, 2017; Published | February 27, 2017
*Correspondence | Dr. S. Bharathy Scientist B, HBSSSPIBD study National Institute of Epidemiology, Indian Council of Medical Research, Chennai, Tamil Nadu, India – 600 077.; Email: drbharathy.vph@gmail.com
Citation | Bharathy S, Gunaseelan L (2017). A Cross Sectional Study To Understanding Demographics Of Dog Bite Victims Attending Anti Rabies Ward In Chennai City, Tamil Nadu India. Adv. Anim. Vet. Sci. 5(2): 78.82.
DOI | http://dx.doi.org/10.14737/journal.aavs/2017/5.2.78.82
ISSN (Online) | 2307-8316; ISSN (Print) | 2309-3331
Copyright © 2017 Bharathy and Gunaseelan. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
INTRODUCTION
Rabies is a disease of antiquity known to man, and still continuous to cause significant mortality. Some of the Asian countries such as Thailand, Philippines and Sri Lanka, have been able to reduce human rabies death but India and neighboring countries such as Pakistan and Bangladesh report thousands of human deaths every year. Human rabies is endemic throughout the mainland India and only the islands of Andaman and Nicobar, Lakshadweep are rabies free (Sudarshan et al., 2007).
The animal mainly responsible for human rabies deaths in India is the dog (96.2%) mostly stray (63%) with majority of rabies deaths occurring in rural areas (91%) (Sudarshan et al., 2007). India has approximately 25 million dogs, with an estimated dog: man ratio of 1:36 (Rahman, 2011) and the dog population in Chennai city was 18,293 in the year 2007 as estimated by Department of Animal Husbandry and Veterinary Services, 18th Livestock Census. Efforts have been made in India to effectively control rabies in dogs (Rahman, 2011). Presently almost 60% of rabies exposed people take one of the modern cell culture vaccines and nearly 5 million doses of these vaccines are sold every year (Sudarshan et al., 2005). The most cost effective strategy for preventing human rabies is the elimination of rabies in dogs through vaccination (WHO, 2001). This study was carried out with the objective of collecting information from victims attending anti rabies ward and relate to the demographics of dog bites identify possible risk factors for human rabies and suggest to improve rabies control measures in Chennai city.
MATERIAL AND METHODS
Study Population and Period
The present cross sectional study was undertaken among the 256 victims of dog bite from different areas of Chennai who attended the anti- rabies ward for post exposure rabies vaccination in three Government General Hospitals of Chennai city between April 2013 and April 2014.
Data Collection Method
The interviewer visited the three government general hospitals in Chennai city weekly once for the purpose of data collection. A pretested and structured oral questionnaire was used to collection the information from the dog bite victims. All the dog bite victims attending these hospitals on a particular day were contacted and explained about the study purpose and each victim interviewed for 10 to 15 minutes. In case of child victim (< 15 years) attendees, preferably parents were explained about the study and information collected thereafter. Invasive procedure and active interventions were not done in the study so only informed verbal consent was taken. They were assured that their responses would be kept secure and confidentiality maintained.
Study Tool Design
Questionnaire was designed to cover various issues regarding exposure to dog bite and the details included briefly demographics, occupation, levels of rabies awareness, category of dog which had bitten (stray dog/pet dog), location of bite wound in body, kind of bite (provoked/unprovoked), type of exposure (bite/scratch/lick), vaccination status of dog, kind of first aid measure that have taken after the dog bite, observation of dogs post bite for 10 days.
The individuals occupation were grouped into; Employee, Business, Unskilled and Student. Provoked bites included chasing the dog, playing, petting, teasing, feeding unfamiliar dog, scolding, hitting, stoning, stamping, bathing, interrupting a dog fight, helping a wounded dog, treating the dog (Veterinarian). Unprovoked bites included absolutely no interaction with the dog prior to bite, territorial behaviour of the dog where the dogs chases motorbikes and cycles and bite the rider, guarding behaviour where house guests were the victims, walking close to a bitch guarding puppies, bites due to fear of fire crackers, pain etc. and presence of other dominant dogs or change of place.
The dogs that bit the victims were classified based on ownership. A dog owned was categorized as pet dog. Those dogs that lived on the streets not under anybody’s care or ownership were categorized as strays.
The wounds of the victims were observed and classified based on the location of the body as lower limb, upper limb, trunk and face. The wounds were also classified based on the degree of wound bite which includes scratch, lick, single bite and multiple bites.
The patients were asked for the location or address of the place where the dog bit them. For mapping the localities where the dog bites were common in Chennai city. Victims were also asked about the vaccination status of the dog that bit them and classified as vaccinated, unvaccinated dog and unknown status. Victims were also asked to relate the present condition of the dog which had inflicted the bite.
RESULTS AND DISCUSSION
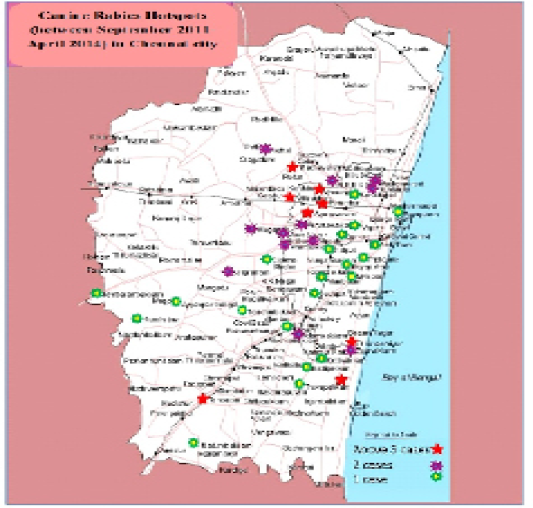
The dog bite victims were largely males (71.87%) in comparison to females (28.13%) (Table 1). This was in agreement with that of (Sudarshan et al., 2007; Shah et al., 2012; Suraweera et al., 2012; Yale et al., 2013). Higher proportion of males could be explained by their activities which was largely outdoor and may frequently bring them in contact with strays. However the major age group of the bite victims were in the 11 to 20 years (21.49%) with 21 to 30 years (20.30%) being second highest (Table 1). Reports from other studies in India indicate children to be vulnerable to have the dogs provoked and less likely to defend themselves (Sudarshan et al., 2007; Shah et al., 2012; Suraweera et al., 2012). The data also revealed that the age groups 11 to 20 years were most susceptible to bites from owned and stray dogs. This could be due to greater interaction of this age group with dogs either as pets.A large proportion of dog bite victims were students (33.97%) followed by unskilled groups (30.08%) (Table 1) again indicating their epidemiological study by (Suraweera et al., 2012) reported 24.3%. Highest victims of dog bites were reported from central part of Chennai as possibly this part Chennai is known to have more number of rabies suspected dogs compared to other parts (Figure 1) which is correlated to the spatial distribution of canine rabies in Chennai city (Figure 2) (Bharathy and Gunaseelan, 2016). Hence people in these areas may be considered to be at a higher risk for dog bites.
In 59.77% of the victims, bite wounds were found on the lower portion of the body (Table 1) which is easily accessible by dogs especially in response to people trampling on them or when dogs chase people during walking or on two wheelers and these findings corroborated with (Sudarshan et al., 2007; Shah et al., 2012; Yale et al., 2013) studies. In the majority of the bite victims the level of exposure were scratches 57.4%, (Table 1) which may not need post bite immunization at all. (Yale et al., 2013) also reported first degree of bites to be more common (74.73%) compared to other type of exposures. Stray dogs accounted for 47% of bite cases, while 53% of victims were bitten by pet dogs (Table 1). In the urban cycle of rabies the risks are more from a free roaming dog population as was also observed by (Yale et al., 2013; Shah et al., 2012).
On the protective status of the dogs only 33.59% were vaccinated, 13.67 % unvaccinated while 52.74 % of victims did not know the vaccination status. Unawareness of vaccination status was reported mostly in stray and community dog bite exposures whereas an equal number of yes and
Table 1: Association of risk factors for human rabies exposure (N= 256)
|

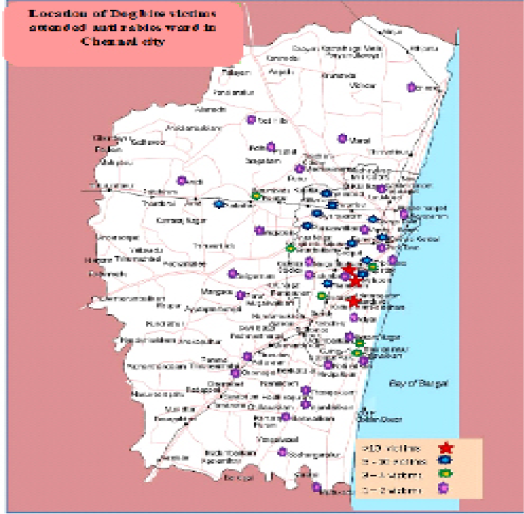
Figure 1: Showing the location of dog bite victims, in which more number of cases has been reported from Central part of Chennai. Red color denotes for more than 10 victims, blue for 5-10 victims, green for 3-4 victims, purple for 1-2 victims.
.
no were received from owned dog bite victims too. This demonstrates that 50% of dog owners did not vaccinate their dogs against rabies being aware of rabies. Around 33.59 % people were bitten by vaccinated apparently healthy pet dogs but came for PEP out of anxiety. To reduce the number of people seeking unnecessary PEP, the public need to be educated.
Table 2: Proportion of people undergoing various post bite protocol
|
Post bite protocols N=256 |
First aid measures |
Time interval for initiation of post exposure immunization |
|||||||
|
Washed wound with only water/soap with water |
Consulted physician |
Unconventional intervention |
Nothing to be done |
< 24 hours |
24-48 hours |
48-72 hours |
73-96 hours |
<96 hours |
|
|
% |
50.78 |
21.86 |
11.72 |
15.63 |
48.44 |
23.05 |
12.89 |
9.76 |
5.86 |
The present study found majority of bites were provoked (60.55%) with only 39.45 per cent being unprovoked (Table 1). (Yale et al., 2013) however observed that only 44.44% bites were provoked and 55.55% were unprovoked. Intentional provocation should be discouraged as unprovoked bites are suspicious for rabies. The study showed that the degree of bite varied significantly with provocation and hence emphasizes the need to educate public in this matter. The dogs which had inflicted the bite were observed for 10 days for rabies disease progression by 72.27 % of victims, in which 69.53 % of observed dogs were healthy and alive after 10 days and only 2.73 % died or were killed (Table 1). An equally similar proportion (74%) of dogs were in a healthy state for 10 days after biting the patient and only 4.74% of the dogs died (Yale et al., 2013). It is known that a rabid dog showing clinical signs will survive for not more than 10 days (Tepsumethanon et al., 2008), hence therefore in 69.53% of the above cases, which had been admitted, were obviously not infectious and hence the person bitten by them did not need the post exposure vaccines.
In present study wound washing was practiced as a first aid measure but only in 51% of the bite victims, 22% consulted a physician, 12% practiced unconventional intervention and 16% did not do anything before taking the post exposure prophylaxis (PEP) (Table 2). In an earlier study approximately 60% of victims had resorted to indigenous treatment following bite (Sudarshan et al., 2007) and 72.5% of victims did not even wash their wounds with soap and water and 52.6% of bite victims had applied indigenous products like chilli powder, snuff etc. which are harmful (Shah et al., 2012). However in this study the number of positives aspects was significantly higher on these practices. Only 48.44% of victims attended the antirabies ward within 24 hours of bite while 23.05% attended on next day for PEP (Table 2). (Shah et al., 2012) reported a slightly higher proportion (68.5%) undergoing PEP within 24 hours. A small proportion that had received rabies vaccine did not complete the full course and the use of rabies immunoglobulin (RIG) was negligible.
The decision to administer and receive either complete or incomplete course of PEP should be based on the dog vaccination history, circumstances of the bite and health outcome of the dogs after the observation period. Strict advice such as vigorous wound washing and immediate medical care following bite, will prevent the development of rabies and curtail the unnecessary use of PEP (Matibag et al., 2007).
CONCLUSION
In conclusion, a larger proportion of dog bite victims were students in the age group of 11-25 years. A majority of the dog bite victims undergo post bite immunization atleast 1 day after bite. A greater proportion of the bites were provoked from owned pet dogs with exposures being very minor (scratch) in majority of cases which may not need post bite immunization at all. However higher dog bite victims were reported from Central part of Chennai and educational campaigns should be focused throughout Chennai city for the community and health care workers about the importance of immediate and adequate post-exposure treatment of rabies and there is a urgent need to start an effective dog population management and immunization program in and around Chennai city.
LIMITATIONS
The subjects included in this study were attending government general Hospitals of Chennai city in Tamil Nadu state, hence study finding can’t be generalized to the whole population at large. To get more insight information generalized epidemiological studies need to be conducted all over the India as well as at community level to know actual demographics of dog bite victims.
ACKNOWLEDGEMENT
The authors are greatly thankful to the TANUVAS University, Chennai for the contribution of the fund for this research work under the Department of Veterinary Public Health and Epidemiology, Madras Veterinary College, Chennai.
AUTHORS’ CONTRIBUTIONS
Both the authors equally contributed in this work by data collection and analysis of the results until manuscript submission.
CONFLICTS OF INTEREST
No conflicts of interest between authors and other institution.
REFERENCES


{kind=link}