Research Journal for Veterinary Practitioners


Case Report

Clinical Management of Lethal Acrodermatitis Syndrome in a Bull Terrier
Verónica Pareja Mena1, Rafael Heredia Cárdenas2, Laura Miranda Contreras2, Camilo Romero Núñez2*
1Universidad de San Francisco de Quito, Diego de Robles s/n, Quito 170157, Ecuador; 2Dermavet Hospital Veterinario, José de la Luz Blanco Mz. 187, Lt.33, Santa Martha Acatitla, Iztapalapa, Ciudad de México.
Abstract | Lethal acrodermatitis is a rare disease of Bull terriers, presumed to be a metabolic disorder of zinc. Is inherited as an autosomal recessive trait. Heretofore, no effective treatment is known and the disease cannot be treated with zinc supplementation in the same way as another dermatosis. Most of the time, the affected animals are euthanized. We describe a dog with lethal acrodermatitis, clinical signs, histopathological characteristics and treatment responses in a Bull Terrier dog. Bull Terriers with lethal acrodermatitis have rare presentations and low casuistry, which is why it is important for clinicians to have knowledge about this disease for a better diagnosis and to enable the better management of lesions and to inform the prognosis to the owners.
Keywords | Zinc deficiency, Hyperkeratosis, Macronychia
Received | March 01, 2021; Accepted | March 26, 2021; Published | March 30, 2021
*Correspondence | Camilo Romero Núñez, Dermavet Hospital Veterinario, José de la Luz Blanco Mz. 187, Lt.33, Santa Martha Acatitla, Iztapalapa, Ciudad de México; Email: mvzcamilo@yahoo.com.mx
Citation | Mena VP, Cardenas RH, Contreras LM, Núñez CR (2021). Clinical management of lethal acrodermatitis syndrome in a bull terrier. Res J. Vet. Pract. 9(1): 9-11.
DOI | http://dx.doi.org/10.17582/journal.rjvp/2021/9.1.9.11
ISSN | 2308-2798
Copyright © 2021 Núñez et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
INTRODUCTION
Zinc is an essential micronutrient with cutaneous antioxidant function. Skin contains approximately 20% of the total reserves of body zinc (Zn) and is especially prevalent in the epidermis. There are different syndromes associated with its deficiency or alterations in assimilation, such as infectious and inflammatory diseases that present cutaneous signs (Beigh et al., 2013; Outerbridge, 2013).
Lethal acrodermatitis (LAD) is a rare disease in bull terrier dogs. It is considered an autosomal recessive inherited disorder of zinc absorption and/or metabolism of unknown aetiology. It shows skin lesions characterised by parakeratotic hyperkeratosis, particularly of the extremities and areas of increased friction, growth retardation, eating difficulties, splayed digits (by abnormal keratinisation), skin, nails (dystrophy and paronychia) (McEwan et al., 2003; Smits et al., 1991) and paws affliction, as well as increased susceptibility to bacterial infections (gastrointestinal tract, respiratory tract and skin) and behavioural abnormalities (McEwan et al., 2000). Occasionally dogs with LAD may have a hard arched palate and abnormal body posture (Gonzalez, 2016). Homozygously affected puppies show clinical signs in the first weeks of life (Outerbridge, 2013) and usually die or have to be euthanised before adulthood (7 months) due to intractable infections (usually bronchopneumonia and sepsis) (Rostaher, 2014). They may also exhibit abnormal behaviour and diarrhoea, although not all of these symptoms are present in all affected puppies (Grider et al., 2007).
Until now, there is no known or no effective treatment, since, LAD does not respond to the oral administration of zinc. Systemic and/or topical antimicrobial therapy is used to treat secondary infections and the use of glucocorticoids may help reduce skin inflammation (McEwan et al., 2000; Rostaher, 2014). Diagnosis is based on clinical signs, physical examination findings, and histopathological findings (Rostaher, 2014). The characteristic histological finding is marked diffuse epidermal/follicular parakeratosis; superficial perivascular dermatitis can be found in all species (Gonzalez, 2016). The objective of this study is to relate the history, clinical signs, histopathological characteristics and treatment response in a bull terrier dog with a diagnosis of lethal acrodermatitis.
Patient Evaluation
History: A three-year-old white coloured, female bull terrier dog weighing 11.5 kg, presented to a dermatological consult for chronic skin problems, with a history of symptoms from 6 months of age. The patient lives in a house, with no other pets. The owner says that the pet has had no vaccinations or deworming treatment. Previously, she was given a series of injections without the knowledge of the owners.
Clinical examination findings: On macroscopic examination, the patient presents hyperkeratosis on the pads of the four limbs, macronychia of all nails of thoracic and pelvic limbs (Figure 1). Clinical examination evaluates a diminished vision, slight delay to stimuli and aggressiveness.

Diagnostic aids: Skin scrapings and trichograms were performed, which were negative, nailfold cytologies were performed in which were positive was obtained for Malassezia, Twenty-eight days later, the patient was sedated and a 6mm punch biopsy was performed on pads, hyperkeratosis and healthy skin; a sample with 2 fragments of tissue (skin with hair and skin), 0.5 cm each (Figure 2), which were analysed by histopathology (Figure 3). Completely removed the hyperkeratosis and the nails were cut, followed by vaccination and deworming.

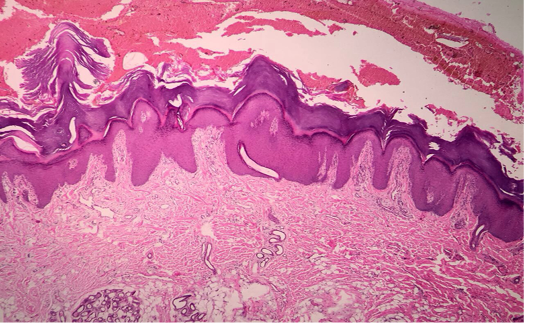
Figure 3: Photomicrography of dermatohistopathological demonstration of marked parakeratotic hyperkeratosis.
Microscopic examination revealed areas of irregular, moderate hyperplasia with compact laminar orthokeratosis and hypergranulosis in the epidermis. At the interface: mild fibrovascular proliferation with poor lymphocytic inflammation.
The result of histopathology of skin fragments and pads: orthokeratotic, moderate, diffuse chronic hyperkeratosis; Mild lymphocytic dermatitis with mild granulation tissue. They suggest familial foot hyperkeratosis.
Treatment approach: The treatment was initiated with vitamin complex with omegas, zinc and copper (Mirrapel®, Comandina, Cali, Colombia), up to 4 ml once a day. Three months later, there was an improvement in 80% of the lesions, exaggerated growth of the nails and decreased weight (10.8kg); the nails were cut and the treatment continue (Mirrapel®). After 4 months, the patient presents a 2/5 body condition, a weight of 9.7 kg and a decrease in muscle mass; the patient’s appetite has not diminished and exaggerated growth of the nails persists. Nails were cut and continuously treated (Mirrapel®).
DISCUSSION AND CONCLUSION
Although it has been reported in other studies that the improvement of lesions caused by this pathology is minimal or even null through the supplementation of either oral or intravenous zinc (Smits et al., 1991), in this study the patient showed an improvement (80%) in skin lesions by the oral supplementation of vitamin complex with omegas, zinc and copper, but with a noticeable decrease in weight.
Until now, most published cases have been reported in puppies, with very few in dogs older than 1 year (McEwan et al., 2000). In contrast, here, we reported a dog of 3 years showing the main dermatological signs for this pathology that result be acrodermatitis, hyperkeratosis and nail symptoms. Currently there are no reports on the use of Mirrapel® as an aid in the management of lethal acrodermatitis bull terrier, only copper and zinc supplementation has been used without obtaining good results, so it is very important further studies.
Currently, genetic tests have been carried out identifying a MKLN1 variant as a candidate causative variant for LAD in Bull Terriers and Miniature Bull Terriers that could aid in the diagnosis of this disease in addition to preventing the involuntary production of dogs affected by LAD (Bauer et al., 2018). However, in the case of this patient it was not possible to perform a genetic analysis, so the diagnosis was based solely on clinical signs and dermatohistopathological demonstration of parakeratotic hyperkeratosis.
Conflict of interest
None.
Author contributions
VPM: Writing - review & editing, Validation, Visualization, Methodology; RHC: Roles/Writing - original draft, Visualization, Investigation; LMC: Investigation, Writing - review & editing, Validation; Visualization, Methodology, Supervision CRN: Conceptualization, Investigation, Resources, Supervision, Validation, Roles/Writing - original draft
REFERENCES